Unilateral Pulmonary Edema: A Rare Initial Presentation of Cardiogenic Shock due to Acute Myocardial Infarction
- Affiliations
-
- 1Division of Cardiology, Hanyang University Guri Hospital, Guri, Korea. leeju@hanyang.ac.kr
- 2Division of Cardiology, Hanyang University Seoul Hospital, Seoul, Korea.
- 3Division of Cardiology, St. Luke's Roosevelt Hospital, New York, NY, USA.
- KMID: 1120161
- DOI: http://doi.org/10.3346/jkms.2012.27.2.211
Abstract
- Cardiogenic unilateral pulmonary edema (UPE) is a rare clinical entity that is often misdiagnosed at first. Most cases of cardiogenic UPE occur in the right upper lobe and are caused by severe mitral regurgitation (MR). We present an unusual case of right-sided UPE in a patient with cardiogenic shock due to acute myocardial infarction (AMI) without severe MR. The patient was successfully treated by percutaneous coronary intervention and medical therapy for heart failure. Follow-up chest Radiography showed complete resolution of the UPE. This case reminds us that AMI can present as UPE even in patients without severe MR or any preexisting pulmonary disease affecting the vasculature or parenchyma of the lung.
Keyword
MeSH Terms
-
Acute Disease
Aged
Coronary Angiography
Diagnosis, Differential
Heart Atria/ultrasonography
Heart Failure/diagnosis/etiology
Humans
Male
Mitral Valve Insufficiency/ultrasonography
Myocardial Infarction/complications/*diagnosis/therapy
Pulmonary Edema/*diagnosis/etiology/therapy
Shock, Cardiogenic/*diagnosis/etiology/therapy
Tomography, X-Ray Computed
Figure
-
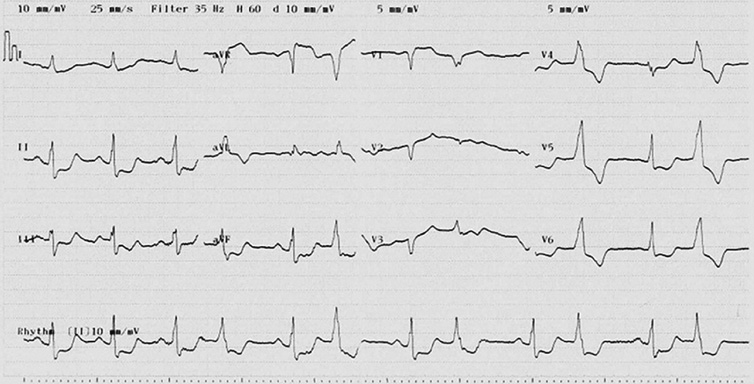
Fig. 1 Initial 12-lead electrocardiogram showing: ST depression in V4-6 and II, III, aVF leads, QS pattern in V1-3 leads, ST elevation in aVR and VPC bigeminy.
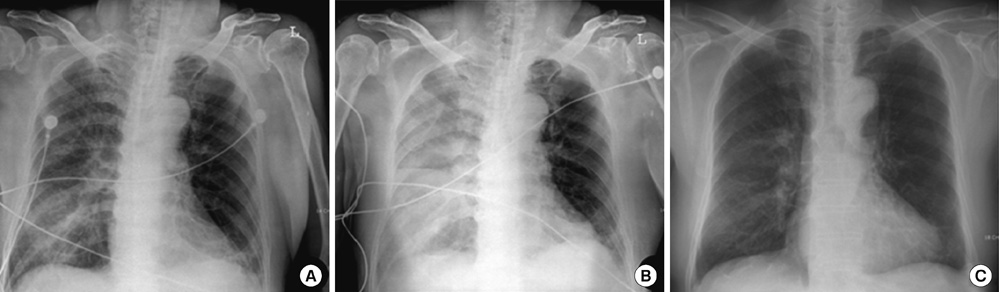
Fig. 2 Chest x-ray. (A) Anteroposterior radiograph of the chest at admission showing alveolar-interstitial infiltrates limited to the right lung. (B) Anteroposterior radiograph of the chest post-successful PCI showing a unilateral homogenous pulmonary opacity occupying the right lobe, and right pleural effusion. (C) Posteroanterior radiograph of the chest at discharge showing complete resolution of the unilateral pulmonary edema.

Fig. 3 Transthoracic echocardiography on admission and four days later after percutaneous coronary intervention (PCI). Echocardiography on admission showing global hypokinesia, mild mitral regurgitation (MR) and left atrium (LA) enlargement (LA volume, 54 mL) (A, B). Four days later after PCI, left ventricular contraction and LA enlargement have improved (LA volume, 34 mL), and MR has resolved (C, D).

Fig. 4 Coronary artery angiography during the primary percutaneous coronary intervention. (A) Left coronary angiography showing significant stenosis from the distal left main coronary artery to the mid left anterior descending artery with thrombolysis in myocardial infarction (TIMI) 2 flow and total occlusion at the ostium of the left circumflex artery with TIMI 0 flow. (B) Final coronary angiography showing successful revascularization without periprocedural complications.

Fig. 5 Computed tomography scan revealing consolidation and ground-glass opacity in the dependent portion of the right lung, with pleural effusion limited to the right lung.
Reference
-
1. Attias D, Mansencal N, Auvert B, Vieillard-Baron A, Delos A, Lacombe P, N'Guetta R, Jardin F, Dubourg O. Prevalence, characteristics, and outcomes of patients presenting with cardiogenic unilateral pulmonary edema. Circulation. 2010. 122:1109–1115.2. Peña C, Jaquet M, Salgado J, Pubul V, Ruibal A, Vázquez B. Asymmetric pulmonary perfusion causing unilateral pulmonary edema as a complication of acute myocardial infarction. Rev Esp Cardiol. 2005. 58:875–877.3. Pena-Gil C, Figueras J, Soler-Soler J. Acute cardiogenic pulmonary edema: relevance of multivessel disease, conduction abnormalities and silent ischemia. Int J Cardiol. 2005. 103:59–66.4. Agarwal R, Aggarwal AN, Gupta D. Other causes of unilateral pulmonary edema. Am J Emerg Med. 2007. 25:129–131.5. Akiyama K, Suetsugu F, Hidai T, Shimamoto K, Takahashi S. Left-sided unilateral pulmonary edema in postinfarction ventricular septal rupture. Chest. 1994. 105:1264–1265.6. Schnyder PA, Sarraj AM, Duvoisin BE, Kapenberger L, Landry MJ. Pulmonary edema associated with mitral regurgitation: prevalence of predominant involvement of the right upper lobe. AJR Am J Roentgenol. 1993. 161:33–36.7. Birnbaum Y, Chamoun AJ, Conti VR, Uretsky BF. Mitral regurgitation following acute myocardial infarction. Coron Artery Dis. 2002. 13:337–344.8. Kyne L, Hausdorff JM, Knight E, Dukas L, Azhar G, Wei JY. Neutrophilia and congestive heart failure after acute myocardial infarction. Am Heart J. 2000. 139:94–100.9. Haeusler KG, Schmidt WU, Foehring F, Meisel C, Guenther C, Brunecker P, Kunze C, Helms T, Dirnagl U, Volk HD, Villringer A. Immune responses after acute ischemic stroke or myocardial infarction. Int J Cardiol. 2010. 10.1016/j.ijcard.2010.10.053.10. D'Aloia A, Faggiano P, Brentana L, Boldini A, Procopio R, Racheli M, Dei Cas L. A difficult diagnosis: right unilateral cardiogenic pulmonary edema. Usefulness of biochemical markers of heart failure for the correct diagnosis. Ital Heart J. 2005. 6:771–774.11. Desjardins VA, Enriquez-Sarano M, Tajik AJ, Bailey KR, Seward JB. Intensity of murmurs correlates with severity of valvular regurgitation. Am J Med. 1996. 100:149–156.12. Piérard LA, Lancellotti P. The role of ischemic mitral regurgitation in the pathogenesis of acute pulmonary edema. N Engl J Med. 2004. 351:1627–1634.13. Raijmakers PG, Bax JJ, Groeneveld AB, Visser FC, Teule GJ, Thijs LG. What is the cause of pulmonary oedema after acute myocardial infarction? A case study. Intensive Care Med. 1996. 22:591–592.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Myocardial Infarction with Cardiogenic Shock in a Young Adult with Minimal Change Disease
- Does arterial hypotension due to cardiogenic shock in older patients lead to functional oliguria or to acute renal failure?
- Intraaortic Balloon Counterpulsation Support in Cardiogenic Shock due to Ventricular Septal Perforation and Huge Inferior Myocardial Infarction
- Mechanical Circulatory Support in the Cardiac Catheterization Laboratory for Cardiogenic Shock
- A Case of Acute Carbon Monoxide Poisoning Resulting in an ST Elevation Myocardial Infarction
