Interventional Management of Gastrointestinal Fistulas
- Affiliations
-
- 1Department of Diagnostic Radiology, Kyung Hee University Medical Center, Seoul, Korea. ohjh6108@hanmail.net
- 2Department of Surgery, Kyung Hee University Medical Center, Seoul, Korea.
- KMID: 1118876
- DOI: http://doi.org/10.3348/kjr.2008.9.6.541
Abstract
- Gastrointestinal (GI) fistulas are frequently very serious complications that are associated with high morbidity and mortality. GI fistulas can cause a wide array of pathophysiological effects by allowing abnormal diversion of the GI contents, including digestive fluid, water, electrolytes, and nutrients, from either one intestine to another or from the intestine to the skin. As an alternative to surgery, recent technical advances in interventional radiology and percutaneous techniques have been shown as advantageous to lower the morbidity and mortality rate, and allow for superior accessibility to the fistulous tracts via the use of fistulography. In addition, new interventional management techniques continue to emerge. We describe the clinical and imaging features of GI fistulas and outline the interventional management of GI fistulas.
Keyword
MeSH Terms
Figure
-
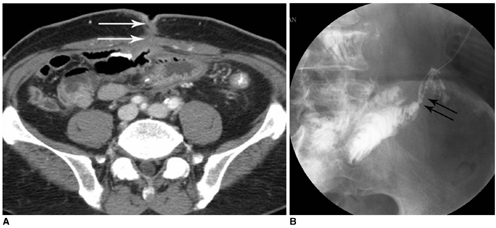
Fig. 1 External fistula after right hemicolectomy due to colon cancer. A. Axial CT image shows jejuno-cutaneous fistula in lower abdomen (arrows). B. Fistulogram using iodinated water-soluble contrast media shows direct communication into jejunal loops (arrows).

Fig. 2 Internal fistula (ileo-colic fistula) in patient with Crohn's disease. A. Three-dimensional reconstruction abdomen CT image shows ileo-colic fistula (arrows). B. In small bowel study, fistula tract between ileum and transverse colon is seen (arrow).

Fig. 3 High-output fistula after Billroth I operation due to stomach cancer. A. Abdomen CT image shows abnormal loculated fluid collection with scanty air-bubbles (arrows) adjacent to gastroduodenal anastomotic site. B. Fistulogram after insertion of drainage tube shows fistula tract (arrow) from intra-abdominal abscess pocket to remnant of stomach via anastomosis site and stenosis at anastomosis site. C. Upper GI series obtained immediately after placement of covered Nitinol stent at gastroduodenal anastomosis site shows fully expanded stent with good passage of contrast media without visible fistula tract. D. Follow-up upper GI series taken three months after stent placement shows properly located stent with excellent patency.
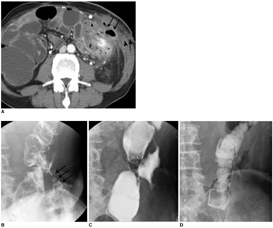
Fig. 4 Low-output, colo-cutaneous fistula with anastomotic stricture in patient with descending colon segmental resection due to trauma. A. Abdominal CT image shows small air-containing abscess pocket (arrows) and subcutaneous fistula tract formation (arrowheads). B. Initial fistulogram shows colo-cutaneous fistula (arrows) with anastomotic stricture at descending colon. C. Placement of covered metallic stent at descending colon anastomosis site. D. Follow-up image obtained after placement of covered metallic stent shows fully expanded stent with good passage of contrast media without visible fistula tract.

Fig. 5 Pancreatico-jejunal fistula in malignant intramural papillary mucinous tumor patient. A. Pancreas shows diffuse pancreatic duct dilatation on US. B. Follow-up three-dimensional reconstruction CT image shows pancreatico-jejunal fistula. Pancreatic duct dilatation is somewhat improved due to this fistula.

Fig. 6 Large abscess formation in mesenteric root after Billroth II operation due to stomach cancer. A. US image shows heterogenous echoic fluid collection (arrows) in mesenteric root. B, C. CT guided 21-gauge needle puncture (B, arrow) and fluoroscopy-guide 10 Fr drainage catheter insertion (C). In C, fistulous tract to third portion of duodenum is observed (arrows).
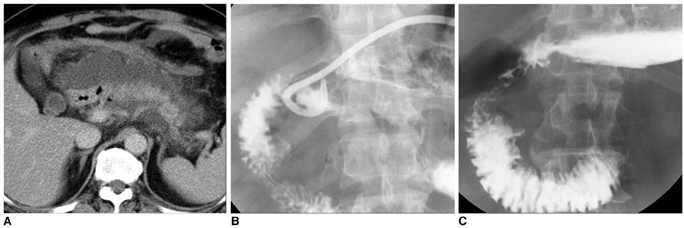
Fig. 7 Percutaneous management of high-output fistulas. A. After Billroth I operation, abdominal CT image shows abnormal fluid collection at anastomotic site and peri-pancreatic portion. B. After drainage of large abscesses, significant decrease in fluid collection is seen. Communication to duodenal bulb is noted. C. Two month follow-up upper GI series shows disappearance of fistulous tract and abscess.

Fig. 8 Transvaginal approach for pelvic abscess drainage. A. 9×5 cm sized abscess cavity (arrows) formation in pelvic cavity following hysterectomy. Fistula tract between sigmoid colon and abscess is observed. B. 8.5 Fr drainage catheter insertion was performed by fluoroscopic guided transvaginal approaches.
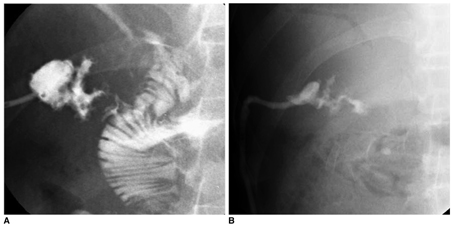
Fig. 9 Fistula located between hepatic abscess and jejunum. A. Tubogram after 8.5 Fr drainage catheter insertion into hepatic abscess shows fistula tract between abscess and jejunum. B. Follow-up tubogram shows decreased abscess size and disappearance of fistula tract to jejunum.

Fig. 10 Jejuno-cutaneous fistula after traffic accident. A. Abdomen CT image shows abscess pocket of approximately 3.9 cm in left upper quadrant (arrows). B. Fistulogram shows jejuno-cutaneous fistula and focal abscess pocket in left upper quadrant. C. Follow-up fistulogram after blockage of fistula tract (arrows) with fibrin glue shows no more visible fistula tracts to jejunal loops.
Reference
-
1. Falconi M, Pederzoli P. The relevance of gastrointestinal fistulae in clinical practice: a review. Gut. 2001. 49:Suppl 4. iv2–iv10.2. Gonzalez-Pinto I, Gonzalez EM. Optimising the treatment of upper gastrointestinal fistulae. Gut. 2001. 49:Suppl 4. iv22–iv31.3. McLean GK, Mackie JA, Freiman DB, Ring EJ. Enterocutaneous fistulae: interventional radiologic management. AJR Am J Roentgenol. 1982. 138:615–619.4. Boverie JH, Remont A. Dondelinger RF, Rossi P, Kurdziel JC, Wallace S, editors. Percutaneous management of fistulas in the digestive tract. Interventional radiology. 1990. Stuttgart: Thieme;746–753.5. Berry SM, Fischer JE. Classification and pathophysiology of enterocutaneous fistulas. Surg Clin North Am. 1996. 76:1009–1018.6. LaBerge JM, Kerlan RK Jr, Gordon RL, Ring EJ. Nonoperative treatment of enteric fistulas: results in 53 patients. J Vasc Interv Radiol. 1992. 3:353–357.7. Han JK. Han MC, Park JH, editors. Percutaneous abdominal abscess drainage. Interventional radiology. 1999. Seoul: Ilchokak;707–714.8. Grunshaw ND, Ball CS. Palliative treatment of an enterorectal fistula with a covered metallic stent. Cardiovasc Intervent Radiol. 2001. 24:438–440.9. Kang YJ, Oh JH, Yoon Y, Kim EJ, Ryu KN, Lim JW, et al. Covered metallic stent placement in the treatment of postoperative fistula resistant to conservative management after Billroth I operation. Cardiovasc Intervent Radiol. 2005. 28:90–92.10. Rabago LR, Ventosa N, Castro JL, Marco J, Herrera N, Gea F. Endoscopic treatment of postoperative fistulas resistant to conservative management using biological fibrin glue. Endoscopy. 2002. 34:632–638.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of interventional radiology in the management of postoperative gastrointestinal leakage
- Interventional radiological approaches to non-variceal gastrointestinal bleeding
- Complications of Arteriovenous Hemodialysis Fistulas: Anglographic Findings and Interventional Treatments
- Over-the-Scope Clip in the Treatment of Gastrointestinal Leaks and Perforations
- The use of OverStitchâ„¢ for the treatment of intestinal perforation, fistulas and leaks
