Respiratory Motion Detection and Correction in ECG-Gated SPECT: a New Approach
- Affiliations
-
- 1Department of Medical Physics, School of Medical Sciences Tarbiat Modares University, Tehran, Iran.
- 2Department of Nuclear Medicine and Endocrinology, PET/CT center, St. Vincent's Hospital, Linz, Austria. mohsen.beheshti@bhs.at
- 3Department of Nuclear Medicine, Rajaei Cardiovascular, Medical and Research Center, Tehran, Iran.
- 4Department of Medical Physics, Iran University, Tehran, Iran.
- 5Department of Nuclear Medicine and Endocrinology, Medical University of Salzburg, Salzburg, Austria.
- KMID: 1118869
- DOI: http://doi.org/10.3348/kjr.2008.9.6.490
Abstract
OBJECTIVE
Gated myocardial perfusion single-photon emission computed tomography (GSPECT) has been established as an accurate and reproducible diagnostic and prognostic technique for the assessment of myocardial perfusion and function. Respiratory motion is among the major factors that may affect the quality of myocardial perfusion imaging (MPI) and consequently the accuracy of the examination. In this study, we have proposed a new approach for the tracking of respiratory motion and the correction of unwanted respiratory motion by the use of respiratory-cardiac gated-SPECT (RC-GSPECT). In addition, we have evaluated the use of RC-GSPECT for quantitative and visual assessment of myocardial perfusion and function. MATERIALS AND METHODS: Twenty-six patients with known or suspected coronary artery disease (CAD)-underwent two-day stress and rest (99m)Tc-Tetrofosmin myocardial scintigraphy using both conventional GSPECT and RC-GSPECT methods. The respiratory signals were induced by use of a CT real-time position management (RPM) respiratory gating interface. A PIO-D144 card, which is transistor-transistor logic (TTL) compatible, was used as the input interface for simultaneous detection of both ECG and respiration signals. RESULTS: A total of 26 patients with known or suspected CAD were examined in this study. Stress and rest myocardial respiratory motion in the vertical direction was 8.8-16.6 mm (mean, 12.4 +/- 2.9 mm) and 7.8-11.8 mm (mean, 9.5 +/- 1.6 mm), respectively. The percentages of tracer intensity in the inferior, inferoseptal and septal walls as well as the inferior to lateral (I/L) uptake ratio was significantly higher with the use of RC-GSPECT as compared to the use of GSPECT (p < 0.01). In a left ventricular ejection fraction (LVEF) correlation analysis between the use of rest GSPECT and RC-GSPECT with echocardiography, better correlation was noted between RC-GSPECT and echocardiography as compared with the use of GSPECT (y = 0.9654x + 1.6514; r = 0.93, p < 0.001 versus y = 0.8046x + 5.1704; r = 0.89, p < 0.001). Nineteen (19/26) patients (73.1%) showed abnormal myocardial perfusion scans with reversible regional myocardial defects; of the 19 patients, 14 (14/26) patients underwent coronary angiography. CONCLUSION: Respiratory induced motion can be successfully corrected simultaneously with the use of ECG-gated SPECT in MPI studies using this proposed technique. Moreover, the use of ECG-gated SPECT improved image quality, especially in the inferior and septal regions that are mostly affected by diaphragmatic attenuation. However, the effect of respiratory correction depends mainly on the patient respiratory pattern and may be clinically relevant in certain cases.
MeSH Terms
-
Aged
Cardiac-Gated Single-Photon Emission Computer-Assisted Tomography/*methods
Coronary Artery Disease/radionuclide imaging
*Coronary Circulation
Electrocardiography
Female
Humans
Male
Middle Aged
Organophosphorus Compounds/diagnostic use
Organotechnetium Compounds/diagnostic use
Radiopharmaceuticals/diagnostic use
*Respiration
Figure
-

Fig. 1 Rejected and accepted cardiac cycles based on respiratory cycle.

Fig. 2 Flowchart of respiratory-cardiac gated single-photon emission computed tomography (RC-GSPECT).

Fig. 3 Respiratory gating equipment mounted on the SPECT system. Real-time position management system, infrared reflective plastic unit, is placed on upper abdomen of patient and camera with infrared illuminator surrounding lens is placed on SPECT bed.

Fig. 4 Comparison of percentage of tracer uptake between use of RC-GSPECT and GSPECT in different left ventricular segments for both rest phase (A) and stress phase (B) study is shown. RC-GSPECT = respiratory-cardiac gated single-photon emission computed tomography, GSPECT = gated myocardial perfusion single-photon emission computed tomography.

Fig. 5 Comparison of ratio of inferior to lateral percent uptake between use of RC-GSPECT and GSPECT in both stress and rest phase studies is shown. RC-GSPECT = respiratory-cardiac gated single-photon emission computed tomography, GSPECT = gated myocardial perfusion single-photon emission computed tomography
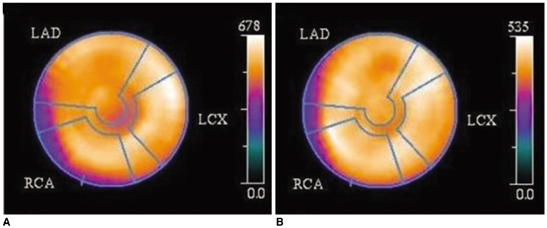
Fig. 6 GSPECT polar map (A) and RC-GSPECT polar map (B) are shown for rest phase study. RC-GSPECT polar map shows increased uptake in inferior wall and septum. RC-GSPECT = respiratory-cardiac gated single-photon emission computed tomography, GSPECT = gated myocardial perfusion single-photon emission computed tomography

Fig. 7 Correlation between LVEF as determined by rest phase GSPECT study and echocardiography (A) and LVEF as determined by rest phase RC-GSPECT study and echocardiography (B). LVEF = left ventricular ejection fraction, RC-GSPECT = respiratory-cardiac gated single-photon emission computed tomography, GSPECT = gated myocardial perfusion single-photon emission computed tomography
Reference
-
1. Germano G, Erel J, Kiat H, Kavanagh PB, Berman DS. Quantitative LVEF and qualitative regional function from gated thallium-201 perfusion SPECT. J Nucl Med. 1997. 38:749–754.2. Go V, Bhatt MR, Hendel RC. The diagnostic and prognostic value of ECG-gated SPECT myocardial perfusion imaging. J Nucl Med. 2004. 45:912–921.3. Segars WP, Tsui BMW. Study of the efficacy of respiratory gating in myocardial SPECT using the new 4-D NCAT. IEEE Trans Nucl Sci. 2002. 49:675–679.4. Tsui BMW, Segars WP, Lalush DS. Effects of upward creep and respiratory motion in myocardial SPECT. IEEE Trans Nucl Sci. 2000. 47:1192–1195.5. Livieratos L, Rajappan K, Stegger L, Schafers K, Bailey DL, Camici PG. Respiratory gating of cardiac PET data in list-mode acquisition. Eur J Nucl Med Mol Imaging. 2006. 33:584–588.6. Wang Y, Riederer SJ, Ehman RL. Respiratory motion of the heart: kinematics and the implications for the spatial resolution in coronary imaging. Magn Reson Med. 1995. 33:713–719.7. Bruyant PP, King MA, Pretorius PH. Correction of the respiratory motion of the heart by tracking of the center of mass of thresholded projections: a simulation study using the dynamic MCAT phantom. IEEE Trans Nucl Sci. 2002. 49:2159–2166.8. Kovalski G, Israel O, Keidar Z, Frenkel A, Sachs J, Azhari H. Correction of heart motion due to respiration in clinical myocardial perfusion SPECT scans using respiratory gating. J Nucl Med. 2007. 48:630–636.9. Pretorius PH, King MA, Tsui BM, LaCroix KJ, Xia W. A mathematical model of motion of the heart for use in generating source and attenuation maps for simulating emission imaging. Med Phys. 1999. 26:2323–2332.10. Berson AM, Emery R, Rodriguez L, Richards GM, Ng T, Sanghavi S, et al. Clinical experience using respiratory gated radiation therapy: comparison of free-breathing and breath-hold techniques. Int J Radiat Oncol Biol Phys. 2004. 60:419–426.11. Fredrickson JO, Wegmuller H, Herfkens RJ, Pelc NJ. Simultaneous temporal resolution of cardiac and respiratory motion in MR imaging. Radiology. 1995. 195:169–175.12. Vedam SS, Keall PJ, Kini VR, Mostafavi H, Shukla HP, Mohan R. Acquiring a four-dimensional computed tomography dataset using an external respiratory signal. Phys Med Biol. 2003. 48:45–62.13. Boucher L, Rodrigue S, Lecomte R, Benard F. Respiratory gating for 3-dimensional PET of the thorax: feasibility and initial results. J Nucl Med. 2004. 45:214–219.14. Cho K, Kumiata S, Okada S, Kumazaki T. Development of respiratory gated myocardial SPECT system. J Nucl Cardiol. 1999. 6:20–28.15. Ehman RL, McNamara MT, Pallack M, Hricak H, Higgins CB. Magnetic resonance imaging with respiratory gating: techniques and advantages. AJR Am J Roentgenol. 1984. 143:1175–1182.16. Kim BH, Ishida Y, Tsuneoka Y, Matsubara N, Hiraoka T, Takeda H, et al. Effects of spontaneous respiration on right and left ventricular function: evaluation by respiratory and ECG gated radionuclide ventriculography. J Nucl Med. 1987. 28:173–177.17. Ohara K, Okumura T, Akisada M, Inada T, Mori T, Yokota H, et al. Irradiation synchronized with respiration gate. Int J Radiat Oncol Biol Phys. 1989. 17:853–857.18. Tada T, Hosono M, Fujioka T, Fukuda H, Nakajima T, Inoue Y. Monitoring of respiratory movement of the diaphragm for gated radiotherapy. Radiat Med. 2005. 23:10–13.19. Pitman AG, Kalff V, Van Every B, Risa B, Barnden LR, Kelly MJ. Effect of mechanically simulated diaphragmatic respiratory motion on myocardial SPECT processed with and without attenuation correction. J Nucl Med. 2002. 43:1259–1267.20. Beach R, Pretorius P, Boening G, Bruyant PP, Feng B, Fulton RR, et al. Feasibility of stereo-infrared tracking to monitor patient motion during cardiac SPECT imaging. IEEE Trans Nucl Sci. 2004. 51:2693–2698.21. Nehmeh SA, Erdi YE, Pan T, Mageras GS, Rosenzweig KE, Schoder H, et al. Quantitation of respiratory motion during 4DPET/ CT acquisition. Med Phys. 2004. 31:1333–1338.22. Nehmeh SA, Erdi YE, Rosenzweig KE, Schoder H, Larson SM, Squire OD, et al. Reduction of respiratory motion artifacts in PET imaging of lung cancer by respiratory correlated dynamic PET: methodology and comparison with respiratory gated PET. J Nucl Med. 2003. 44:1644–1648.23. O'Dell WG, Moore CC, Hunter WC, Zerhouni EA, McVeigh ER. Three-dimensional myocardial deformations: calculation with displacement field fitting to tagged MR images. Radiology. 1995. 195:829–835.24. Chin BB, Nakamoto Y, Kraitchman DL, Marshall L, Wahl R. PET-CT evaluation of 2-deoxy-2-[18F]fluoro-D-glucose myocardial uptake: effect of respiratory motion. Mol Imaging Biol. 2003. 5:57–64.25. Pillay M, Cox PH, Schonfeld DH, Mathews S. Tc-99m tetrofosmin myocardial distribution 4 hours post injection. Int J Card Imaging. 1996. 12:127–135.26. Slomka PJ, Nishina H, Abidov A, Hayes SW, Friedman JD, Berman DS, et al. Combined quantitative supine-prone myocardial perfusion SPECT improves detection of coronary artery disease and normalcy rates in women. J Nucl Cardiol. 2007. 14:44–52.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- New Imaging Technique in Myocardial Perfusion SPECT
- Transient Prolonged Stunning by Dipyridamole Stress Proved by Post-stress ( 1 hour ) and 24 hour Tc-99m-MIBI Gated SPECT
- Assessment of Ventricular Function Using Gated Blood Pool Scan and Gated Blood Pool SPECT
- Performance of Gated Myocardial Perfusion SPECT to Diagnose Coronary Artery Disease
- Gated Myocardial SPECT
