Where Does It Lead? Imaging Features of Cardiovascular Implantable Electronic Devices on Chest Radiograph and CT
- Affiliations
-
- 1Department of Diagnostic and Interventional Radiology, University of Duesseldorf, Medical Faculty, 40225 Dusseldorf, Germany. pkroepil@gmx.de
- 2Department of Cardiovascular Surgery, University Hospital Dusseldorf, 40225 Dusseldorf, Germany.
- 3Department of Radiology, Massachusetts General Hospital, Boston, MA 02114, USA.
- KMID: 1116447
- DOI: http://doi.org/10.3348/kjr.2011.12.5.611
Abstract
- Pacemakers and implantable cardioverter defibrillators (ICDs) are being increasingly employed in patients suffering from cardiac rhythm disturbances. The principal objective of this article is to familiarize radiologists with pacemakers and ICDs on chest radiographs and CT scans. Therefore, the preferred lead positions according to pacemaker types and anatomic variants are introduced in this study. Additionally, the imaging features of incorrect lead positions and defects, as well as complications subsequent to pacemaker implantation are demonstrated herein.
Keyword
- Pacemaker; ICD; Chest; Radiograph; CT
MeSH Terms
Figure
-
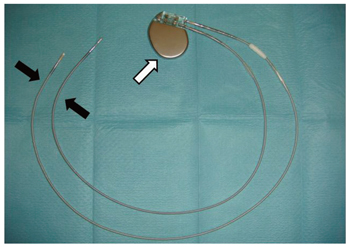
Fig. 1 Cardiovascular implantable electronic devices consists of one or more leads (black arrows) connected to pulse generator (white arrow).
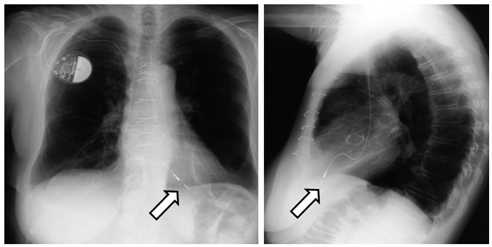
Fig. 2 75-year-old female patient with single lead ventricular pacemaker (VVI). Posteroanterior (PA) and lateral chest radiographs show preferred tip position in apex of right ventricle (arrows).
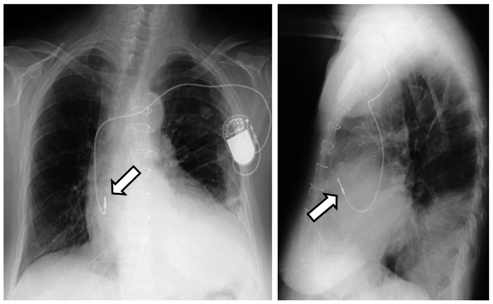
Fig. 3 72-year-old female patient with single lead atrial pacemaker (AAI). PA and lateral chest radiographs show preferred tip position in right atrial appendage (arrows). Note that lead typically curves superiorly and anteriorly into atrial appendage.

Fig. 4 57-year-old female patient with two-lead bichamber pacemaker (DDD). Preferred tip position is right atrial appendage (white arrows) and apex of right ventricle (black arrows), as seen on PA and lateral chest radiographs.

Fig. 5 69-year-old male patient with biventricular pacemaker (CRT). PA and lateral chest radiographs show preferred tip position in right atrial appendage (white arrows), apex of right ventricle (black arrows), and in posterior coronary vein at left ventricle (arrowheads).
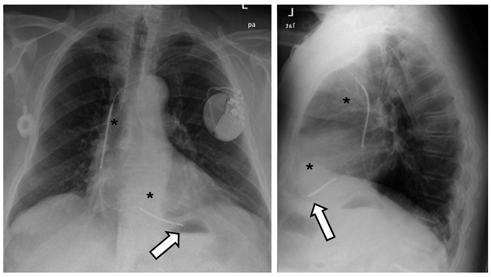
Fig. 6 67-year-old patient with implantable cardioverter defibrillator (ICD). PA and lateral chest radiographs demonstrate preferred tip location in apex of right ventricle (white arrows). Implantable cardioverter defibrillator leads contain one or two coils (*) to enable delivery of energy to myocardium. Proximal coil typically resides within superior vena cava. Note that lead tracks along base of right atrium, curves superiorly as it transverses tricuspid valve, and then turns inferiorly as it enters right ventricle.

Fig. 7 77-year-old male patient with persistent left superior vena cava following implantation of dual-chamber implantable cardioverter defibrillator. Right atrium and ventricle are reached via coronary sinus. Note superior vena cava lead (arrows) in persistent left superior vena cava.

Fig. 8 53-year-old male patient with DDD pacemaker following mitral and tricuspidal valve annuloplasties. PA and lateral chest radiographs show that right ventricular lead (arrowheads) can traverse tricuspid annuloplasty (arrows).
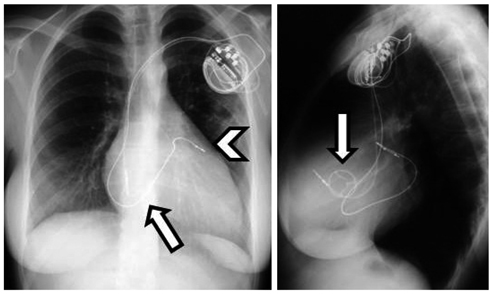
Fig. 9 69-year-old female patient after mechanical tricuspidal valve replacement (TVR, arrows). In this case, placement of ventricular lead (arrowhead) should be via coronary sinus, as seen on PA and lateral chest radiographs.

Fig. 10 21-year-old male patient with dual-chamber implantable cardioverter defibrillator following Mustard procedure to correct for transposition of great arteries. Scheme (B) and CT scan performed prior to implantable cardioverter defibrillator placement (C-E) show cardiovascular anatomy. Baffle was constructed to direct venous blood to left atrium (B). Oxygenated blood from pulmonary veins is directed to right atrium (RA) and from there to systemic right ventricle (RV) (B-E). PA and lateral chest radiographs (A) demonstrate leads that course from left brachiocephalic vein into anatomical left atrium (functional right atrium, arrowhead) and into anatomical left ventricle (LV) (functional right ventricle).

Fig. 11 77-year-old male patient with dual-chamber implantable cardioverter defibrillator. Initial PA and lateral chest radiographs (A) show displacement of atrial lead (white arrows) into right ventricle. After revision, PA and lateral radiographs (B) show correct lead position in right atrium (black arrows). Note epimyocardial lead over right ventricle (*).
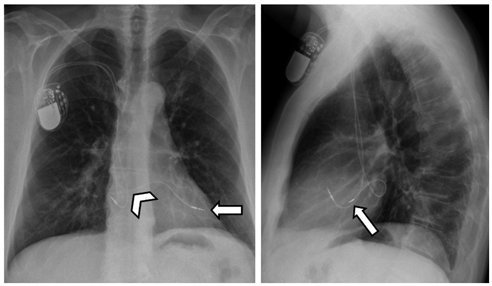
Fig. 12 61-year-old male patient with atrial septal defect following implantation of DDD pacemaker. PA and lateral chest radiographs demonstrate correct position of right atrium lead, whereas ventricular lead curves superiorly and to left just above level of right atrial lead (arrowhead). This course is typical for malpositioned lead traversing from right atrium to left atrium via atrial septal defect and then into left ventricle (arrows).

Fig. 13 77-year-old male patient with DDD pacemaker. PA chest radiograph shows superiorly facing ventricular lead tip, which is suggestive of malposition in coronary sinus (arrow in PA radiograph). Malposition in coronary sinus over left ventricle is confirmed on lateral radiograph (arrow).

Fig. 14 35-year-old male patient after implantation of DDD pacemaker. PA and lateral chest radiographs show loop of ventricular lead in right ventricular outflow tract (arrows), which caused insufficiency of pulmonary valve.

Fig. 15 42-year-old male patient with Twiddler syndrome. Initial PA radiograph shows preferred lead position and generator configuration of single lead ventricular pacemaker (VVI) (A). Several months later, winding of pacemaker lead around generator can be seen on PA chest radiograph (B), causing dislodgement of ventricular lead (arrow).
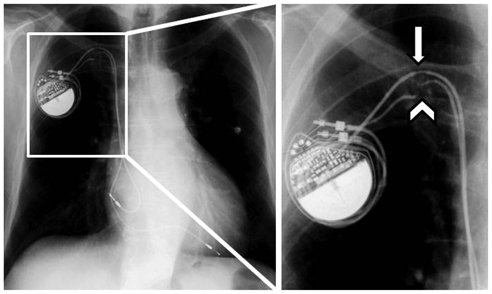
Fig. 16 52-year-old male patient with DDD pacemaker. PA chest radiograph shows fracture (arrowhead) of ventricle lead and insulation breach (arrow) of atrial lead in subclavian vein adjacent to clavicle ("subclavian crush syndrome").
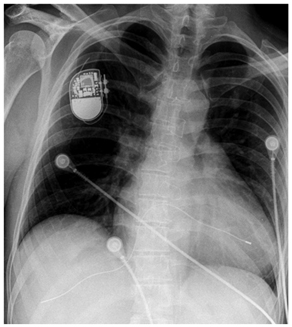
Fig. 17 59-year-old male with single ventricular lead pacemaker. PA chest radiograph discloses lead fracture and dislodgement of lead fragment into hepatic vein.

Fig. 18 82-year-old female patient with DDD pacemaker. Sagittal (A) and transverse (B) CT reconstructions show perforation of atrial pacemaker lead (arrow) with development of significant hemopericardium (*).

Fig. 19 59-year-old male patient following DDD pacemaker implantation. Hematopneumothorax (arrows) is seen on PA and lateral chest radiographs on contralateral side of pacemaker generator (A). Additional CT scan confirms hematopneumothorax (B, *) and shows perforation of atrial lead (arrowheads in B, C). (Courtesy of Dr. Keske, Gelsenkirchen, Germany).
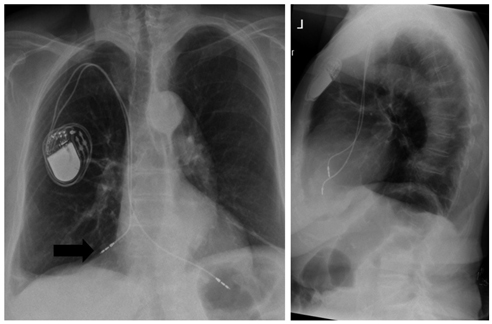
Fig. 20 84-year-old female patient with DDD pacemaker. Perforation of atrial pacemaker lead is seen on PA chest radiograph (arrow).
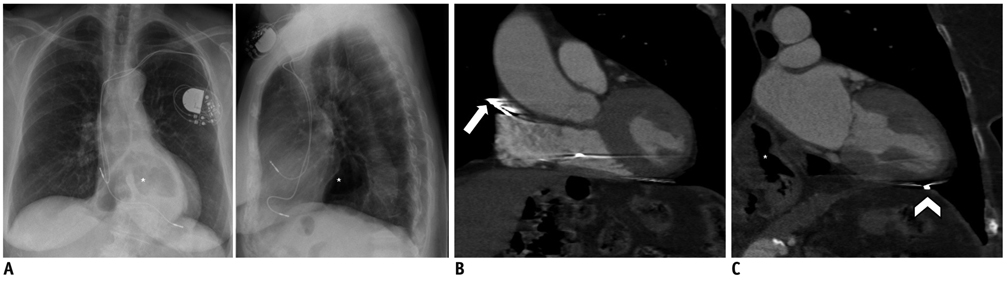
Fig. 21 84-year-old female patient with DDD pacemaker suffering from diaphragmatic stimulation. PA and lateral chest radiographs (A) indicate correct lead positions. However, asymptomatic perforation of atrial (arrow) and ventricular (arrowhead) lead is seen on contrast-enhanced CT scans (B, C). Note upside-down stomach (*).
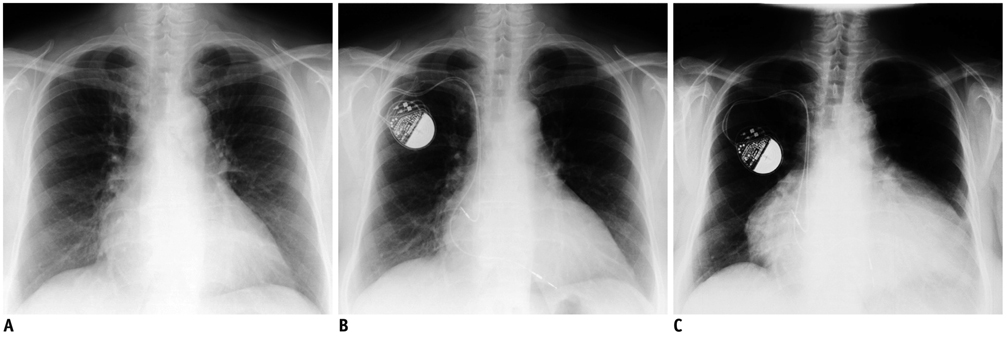
Fig. 22 61-year-old female suffering from postcardiotomy syndrome. PA chest radiograph of 61-year-old female patient prior to pacemaker implantation shows regular heart size (A). Correct lead position is seen immediately following implantation of DDD pacemaker (B). Three months later, patient suffered from fever and poor cardiac function. Massive pericardial effusion was observed seen on PA chest radiograph (C), which was attributed to postcardiotomy syndrome.
Reference
-
1. Borek PP, Wilkoff BL. Pacemaker and ICD leads: strategies for long-term management. J Interv Card Electrophysiol. 2008. 23:59–72.2. Grier D, Cook PG, Hartnell GG. Chest radiographs after permanent pacing. Are they really necessary? Clin Radiol. 1990. 42:244–224.3. Heldman D, Mulvihill D, Nguyen H, Messenger JC, Rylaarsdam A, Evans K, et al. True incidence of pacemaker syndrome. Pacing Clin Electrophysiol. 1990. 13:1742–1750.4. Markewitz A. [Yearly report for 2007 of the German Pacemaker registry]. Herzschrittmacherther Elektrophysiol. 2008. 19:195–223.5. Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004. 350:2140–2150.6. Connolly SJ, Hallstrom AP, Cappato R, Schron EB, Kuck KH, Zipes DP, et al. Meta-analysis of the implantable cardioverter defibrillator secondary prevention trials. AVID, CASH and CIDS studies. Antiarrhythmics vs Implantable Defibrillator study. Cardiac Arrest Study Hamburg. Canadian Implantable Defibrillator Study. Eur Heart J. 2000. 21:2071–2078.7. Ratliff HL, Yousufuddin M, Lieving WR, Watson BE, Malas A, Rosencrance G, et al. Persistent left superior vena cava: case reports and clinical implications. Int J Cardiol. 2006. 113:242–246.8. Jokinen JJ, Turpeinen AK, Pitkanen O, Hippelainen MJ, Hartikainen JE. Pacemaker therapy after tricuspid valve operations: implications on mortality, morbidity, and quality of life. Ann Thorac Surg. 2009. 87:1806–1814.9. Moons P, Gewillig M, Sluysmans T, Verhaaren H, Viart P, Massin M, et al. Long term outcome up to 30 years after the Mustard or Senning operation: a nationwide multicentre study in Belgium. Heart. 2004. 90:307–313.10. Pakarinen S, Oikarinen L, Toivonen L. Short-term implantation-related complications of cardiac rhythm management device therapy: a retrospective single-centre 1-year survey. Europace. 2010. 12:103–108.11. Wiegand UK, LeJeune D, Boguschewski F, Bonnemeier H, Eberhardt F, Schunkert H, et al. Pocket hematoma after pacemaker or implantable cardioverter defibrillator surgery: influence of patient morbidity, operation strategy, and perioperative antiplatelet/anticoagulation therapy. Chest. 2004. 126:1177–1186.12. Burney K, Burchard F, Papouchado M, Wilde P. Cardiac pacing systems and implantable cardiac defibrillators (ICDs): a radiological perspective of equipment, anatomy and complications. Clin Radiol. 2004. 59:699–708.13. Aggarwal RK, Connelly DT, Ray SG, Ball J, Charles RG. Early complications of permanent pacemaker implantation: no difference between dual and single chamber systems. Br Heart J. 1995. 73:571–575.14. Edwards NC, Varma M, Pitcher DW. Routine chest radiography after permanent pacemaker implantation: is it necessary? J Postgrad Med. 2005. 51:92–96. discussion 96-97.15. Castillo R, Cavusoglu E. Twiddler's syndrome: an interesting cause of pacemaker failure. Cardiology. 2006. 105:119–121.16. Magney JE, Flynn DM, Parsons JA, Staplin DH, Chin-Purcell MV, Milstein S, et al. Anatomical mechanisms explaining damage to pacemaker leads, defibrillator leads, and failure of central venous catheters adjacent to the sternoclavicular joint. Pacing Clin Electrophysiol. 1993. 16:445–457.17. Connolly SJ, Gent M, Roberts RS, Dorian P, Roy D, Sheldon RS, et al. Canadian implantable defibrillator study (CIDS) : a randomized trial of the implantable cardioverter defibrillator against amiodarone. Circulation. 2000. 101:1297–1302.18. Roelke M, O'Nunain SS, Osswald S, Garan H, Harthorne JW, Ruskin JN. Subclavian crush syndrome complicating transvenous cardioverter defibrillator systems. Pacing Clin Electrophysiol. 1995. 18:973–979.19. Mahapatra S, Bybee KA, Bunch TJ, Espinosa RE, Sinak LJ, McGoon MD, et al. Incidence and predictors of cardiac perforation after permanent pacemaker placement. Heart Rhythm. 2005. 2:907–911.20. Kiviniemi MS, Pirnes MA, Eranen HJ, Kettunen RV, Hartikainen JE. Complications related to permanent pacemaker therapy. Pacing Clin Electrophysiol. 1999. 22:711–720.21. Ho WJ, Kuo CT, Lin KH. Right pneumothorax resulting from an endocardial screw-in atrial lead. Chest. 1999. 116:1133–1134.22. Hirschl DA, Jain VR, Spindola-Franco H, Gross JN, Haramati LB. Prevalence and characterization of asymptomatic pacemaker and ICD lead perforation on CT. Pacing Clin Electrophysiol. 2007. 30:28–32.23. Snow ME, Agatston AS, Kramer HC, Samet P. The postcardiotomy syndrome following transvenous pacemaker insertion. Pacing Clin Electrophysiol. 1987. 10:934–936.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Experiences of magnetic resonance imaging scanning in patients with pacemakers or implantable cardioverter-defibrillators
- Cardiac Implantable Electronic Devices and Magnetic Resonance Imaging
- Hematoma Prevention Using Tachosil (Fibrin Sealant) Patch during Insertion of Cardiovascular Implantable Electronic Devices without Suspending Antithrombotics: Three Case Reports
- Efforts of the Past 20 Years for Proved Magnetic Resonance Imaging Safety of Medtronic Implantable Cardiac Devices
- Cardiac Implantable Electronic Device Safety during Magnetic Resonance Imaging
