Clinico-Radiologic Findings of Entrapped Inferior Oblique Muscle in a Fracture of the Orbital Floor
- Affiliations
-
- 1Department of Ophthalmology, Korea University College of Medicine, Ansan Hospital, Ansan, Korea. ansaneye@hanmail.net
- 2Department of Diagnostic Radiology, Korea University College of Medicine, Ansan Hospital, Ansan, Korea.
- KMID: 1115759
- DOI: http://doi.org/10.3341/kjo.2009.23.3.224
Abstract
- A 51-year old man presented with vertical and torsional diplopia after reduction of a blowout fracture at another hospital one year ago. He had no anormalies of head position and 14 prism diopters (PD) right hypertropia (RHT) in the primary position. In upgaze no vertical deviation was found, and hyperdeviation on downgaze was 35PD. Bielschowsky head tilt test showed a negative response. Distinct superior oblique (SO) and inferior rectus (IR) underaction of the right eye was noted but IO overaction was mild on the ocular version test. Double Maddox rod test (DMRT) revealed 10-degree extorsion, but fundus extorsion was minimal in the right eye.Thin-section coronal CT scan showed that there was no fracture line on the anterior orbital floor, but a fracture remained on the posterior orbital floor. Also, the anterior part of the right inferior oblique muscle was vertically reoriented and the medial portion of the inferior oblique muscle was not traced on the coronal CT scan. The patient underwent 14 mm right IO recession and 3 mm right IR resection. One month after the surgery, his vertical and torsional diplopia were eliminated in the primary position.
Keyword
MeSH Terms
Figure
-
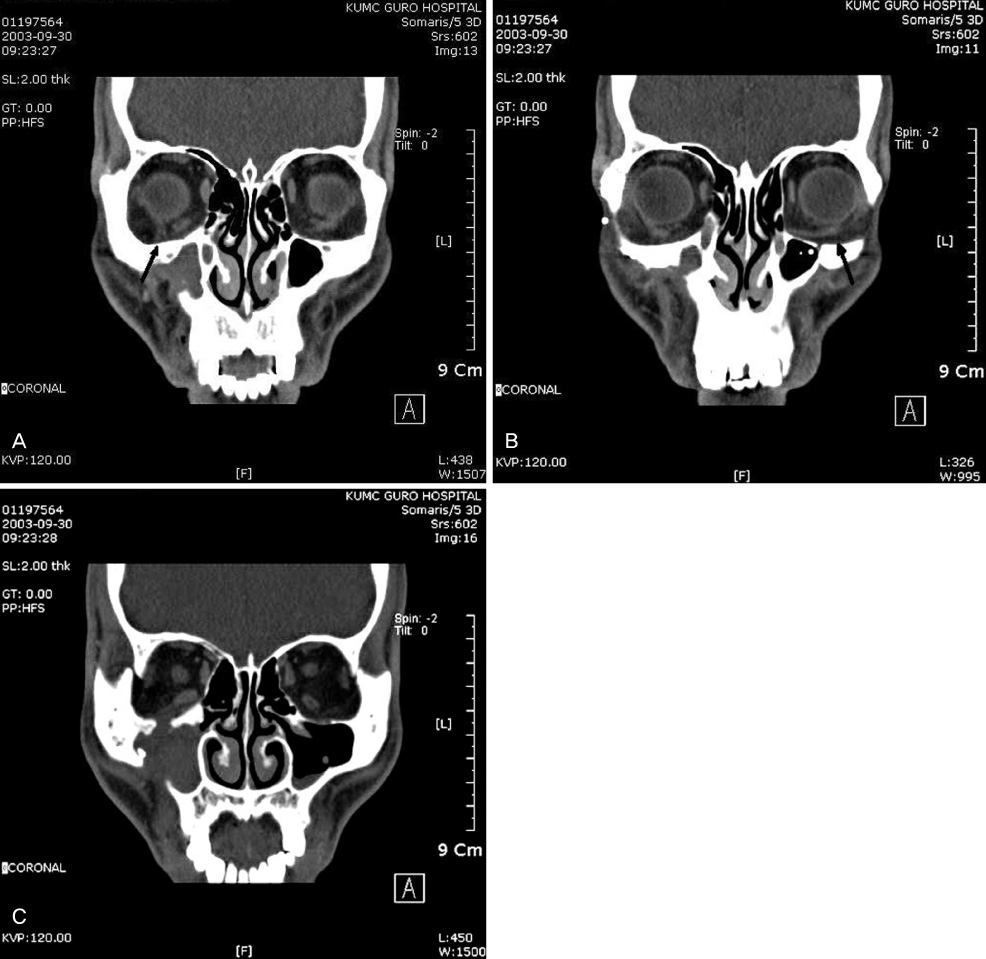
Fig. 1 Preoperative coronal CT revealed an intact anterior right orbital floor and the inferior oblique muscle, which is vertically oriented at the globe attachment portion in the right eye. The inferior oblique muscle exhibits a thick and irregular appearance (arrow) (A). The medial portion is not traced. Note the normal inferior oblique muscle in the left eye (arrow) (B). The fractured posterior right orbital floor is also noted (C).
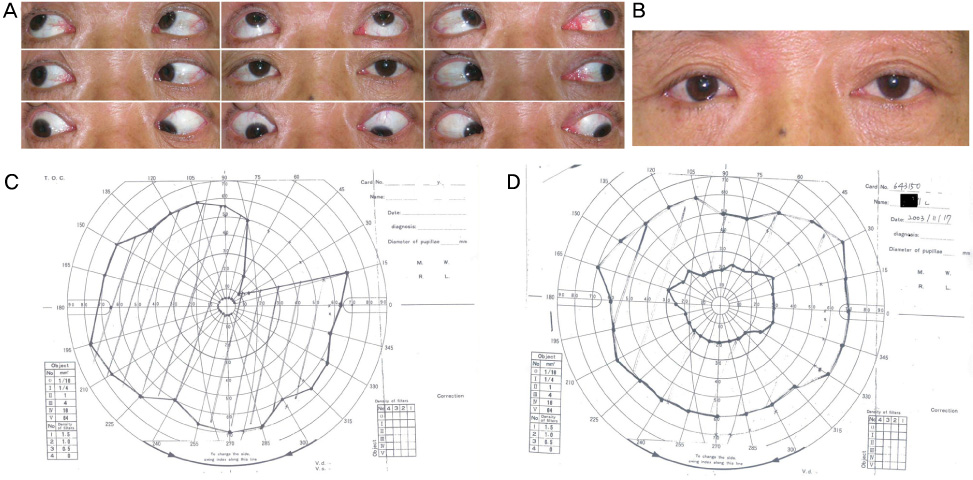
Fig. 2 (A) Nine cardinal movement of the eyeball on preoperative day. Right hypertropia is noted at primary position. Mild inferior oblique overaction and significant limitation on downward gaze of the right eye are noted. (B) Orthophoria on the primary position is observed one month after surgery. (C) Single binocular visual field upon preoperative examination (patient view). Diplopia-free field is limited in the right superior temporal field. (D) Single binocular visual field one month after surgery (patient view). The patient's single binocular visual field expands into the primary gaze and downgaze.
Reference
-
1. Metz HS, Scott WE, Madson E, Scott AB. Saccadic velocity and active force studies in blow-out fractures of orbit. Am J Ophthalmol. 1974. 78:665–670.2. Cole HG, Smith B. Eye muscle imbalance complicating orbital floor fractures. Am J Ophthalmol. 1963. 55:930–935.3. Seiff SR, Good WV. Hypertropia and the posterior blowout fracture. Ophthalmology. 1996. 103:152–156.4. Nardi M. Hypertropia and the posterior blowout fracture. Ophthalmology. 1996. 103:995–996.5. Parks MM. Inferior oblique weakening procedures. Int Ophthalmol Clin. 1985. 25:107–117.6. Rosenbaum AL, Santiago AP. Clinical strabismus management Principles and Surgical Techniques. 1999. 1st ed. Philadelphia: W.B. Saunders;309–319.7. Ruttum MS, Harris GJ. Orbital blowout fracture with ipsilateral fourth nerve palsy. Am J Ophthalmol. 1985. 100:343–344.8. Parks MM. Isolated cyclovertical muscle palsy. AMA Arch Ophthalmol. 1958. 60:1027–1035.9. Veronneau-Troutman S. A four-step test for diagnosis of pseudo superior oblique palsy. Graefes Arch Clin Exp Ophthalmol. 1988. 226:317–322.10. Plager DA. Tendon laxity in superior oblique palsy. Ophthalmology. 1992. 99:1032–1038.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Study on the Anatomical Position of the Inferior Oblique Muscle Insertion in Primary Inferior Oblique Overaction
- The Effect of Anteriorization of The Inferior Oblique Muscle in +3 or +4 Inferior Oblique Overaction
- The Case of Inferior Oblique Muscle Overaction after Orbital Trauma
- Secondary Superior Oblique Overaction after Inferior Oblique Muscle Myectomy in a Patient Misdiagnosed with Inferior Oblique Muscle Overaction
- The Effect of Modified Anterior Transposition of the Inferior Oblique Muscle for Hypertropia in Superior Oblique Muscle Palsy with Inferior Oblique Muscle Overaction
