Ruptured Epidermal Inclusion Cysts in the Subareolar Area: Sonographic Findings in Two Cases
- Affiliations
-
- 1Department of Radiology, Uijongbu St. Mary's Hospital, Catholic University College of Medicine, Kyunggido, Korea. tiger@catholic.ac.kr
- 2Department of Radiology, Kangnam St. Mary's Hospital, Catholic University College of Medicine, Seoul , Korea.
- 3Department of Surgery, Uijongbu St. Mary's Hospital, Catholic University College of Medicine, Kyunggido, Korea.
- 4Department of Clinical Pathology, Uijongbu St. Mary's Hospital, Catholic University College of Medicine, Kyunggido, Korea.
- KMID: 1110735
- DOI: http://doi.org/10.3348/kjr.2007.8.4.356
Abstract
- Epidermal inclusion cyst of the breast is an uncommon benign lesion and it is usually located in the skin layer. We report here on two cases of ruptured epidermal inclusion cysts in the subareolar area, which is a very unusual location for these cysts and these lesions can be mistaken for breast malignancies.
MeSH Terms
Figure
-
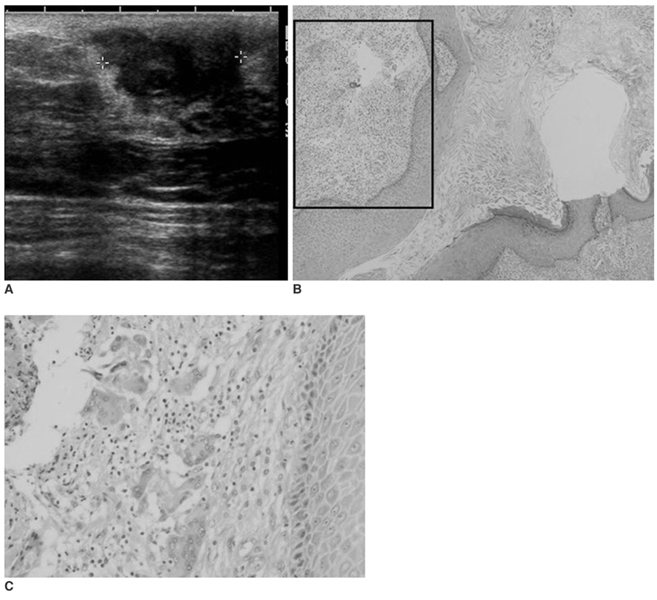
Fig. 1 A 50-year-old woman with a palpable left subareolar mass. A. Sonography shows a heterogeneoulsy hypoechoic mass with an indistinct margin. B. Photomicrograph shows that the lesion is lined by epidermal-type epithelium and it is filled with keratinous material, which is pathognomonic for an epidermal inclusion cyst. (Hematoxylin & Eosin staining × 40) C. Photomicrograph of adjacent tissue (box in B) reveals inflammatory infiltrate cells or a foreign body reaction. (Hematoxylin & Eosin staining × 100)
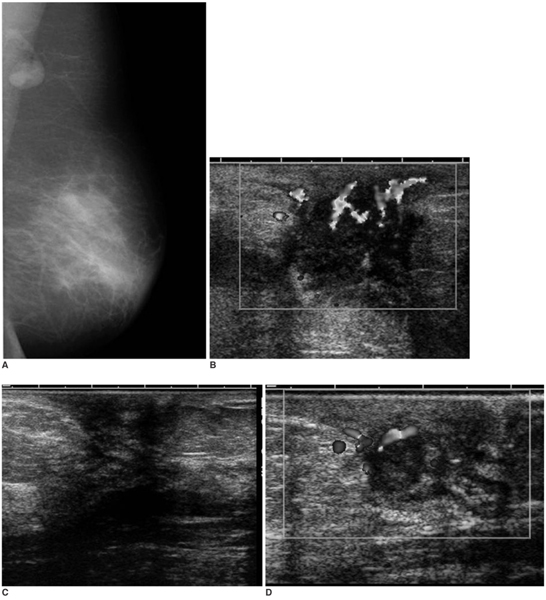
Fig. 2 A 44-year-old woman with periareolar pain of the left breast. A-D. The initial mediolateral oblique mammogram shows asymmetry of the left subareolar area, periareolar skin thickening and axillary lymphadenopathy (A), and the initial sonography shows a heterogeneous mass with peripherally increased vascular flow (B). About one year after medical treatment, the mass disappeared on sonography with a remaining Ill defined low echoic subareolar portion (C). The discrete subareolar mass was again noted seven months later on sonography when she revisited the hospital with a heat sensation and tenderness (D).
Reference
-
1. Kwak JY, Park HL, Kim JY, Kim EK, Chung SY, Kwon TH, et al. Imaging findings in a case of epidermal inclusion cyst arising within the breast parenchyma. J Clin Ultrasound. 2004. 32:141–143.2. Fajardo LL, Bessen SC. Epidermal inclusion cyst after reduction mammoplasty. Radiology. 1993. 186:103–106.3. Denison CM, Ward VL, Lester SC, DiPiro PJ, Smith DN, Meyer JE, et al. Epidermal inclusion cysts of the breast: three lesions with calcifications. Radiology. 1997. 204:493–496.4. Gerlock AJ. Epidermal inclusion cyst of the breast associated with needle biopsy. Radiology. 1974. 112:69–70.5. Hasleton PS, Misch KA, Vasudev KS, George D. Squamous carcinoma of the breast. J Clin Pathol. 1978. 31:116–124.6. Stephenson TJ, Cotton DWK. Paget's disease in an epidermal cyst. Dermatologica. 1987. 174:186–190.7. Crowe DJ, Helvie MA, Wilson TE. Breast infection Mammographic and sonographic findings with clinical correlation. Invest Radiol. 1995. 30:582–587.8. Giess CS, Keating DM, Osborne MP, Ng YY, Rosenblatt R. Retroareolar breast carcinoma: clinical, imaging, and histopathologic features. Radiology. 1998. 207:669–673.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Ruptured Epidermal Inclusion Cyst in the Breast Presenting as a Recurrent Abscess
- Ruptured Epidermal Inclusion Cyst in the Axilla: A Case Report
- Usefulness of Ultrasonography in Differential Diagnosis between Ruptured and Unruptured Epidermal Cysts
- Epidermal Cyst of the Breast Simulating a Benign Solid Mass: A Case Report
- Chronic and Recurrent Subareolar Abscess of the Breast from Underlying Causes
