Differentiation of Adrenal Adenoma and Nonadenoma in Unenhanced CT: New Optimal Threshold Value and the Usefulness of Size Criteria for Differentiation
- Affiliations
-
- 1Department of Diagnostic Radiology and Research Institute of Radiological Science, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. kimnex@yumc.yonsei.ac.kr
- 2Institute of Gastroenterology and Brain Korea 21 project, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1110730
- DOI: http://doi.org/10.3348/kjr.2007.8.4.328
Abstract
OBJECTIVE
To determine the optimal threshold for the attenuation values in unenhanced computed tomography (CT) and assess the value of the size criteria for differentiating between an adrenal adenoma and a nonadenoma. MATERIALS AND METHODS: The unenhanced CT images of 45 patients at our institution, who underwent a surgical resection of an adrenal masses between January 2001 and July 2005, were retrospectively reviewed. Forty-five adrenal masses included 25 cortical adenomas, 12 pheochromocytomas, three lymphomas, and five metastases confirmed by pathology were examined. The CT images were obtained at a slice thickness of 2 mm to 3 mm. The mAs were varied from 100 to 160 and 200 to 280, while the 120 KVp was maintained in all cases. The mean attenuation values of an adrenal adenoma and nonadenoma were compared using an unpaired t test. The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy at thresholds of 10 HU, 20 HU, and 25 HU were compared. The diagnostic accuracy according to the size criteria from 2 cm to 6 cm was also compared. RESULTS: The twenty-five adenomas showed significantly lower (p < 0.05) attenuation values (mean+/-SD; 16.3+/-14.9) than the nonadenomas (38.1+/-6.8). Nineteen (90%) of the 20 nonadenomas had attenuation values ranging from 30 to 50 HU. The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for diagnosing adenomas were 36%, 100%, 100%, 56%, and 64%, respectively, at a threshold of 10 HU; 60%, 100%, 100%, 67%, and 78%, respectively, at a threshold of 20 HU; and 72%, 95%, 95%, 73%, and 82%, respectively, at a threshold of 25 HU. The adenomas had a significantly (p < 0.05) smaller diameter (2.44+/-1.24 cm) than the nonadenomas (5.09 +/- 2.37 cm). The size criteria using a diameter of 4-6 cm showed a sensitivity > 90% but a specificity < 70%. Size criteria of 2 or 3 cm had a high specificity of 100% and 80% but a low sensitivity of 20% and 60%. CONCLUSION: The threshold attenuation values of 20 or 25 HU in the unenhanced CT appear optimal for discriminating an adrenal adenoma from a nonadenoma. The size criteria are of little value in differentiating adrenal masses because of their low specificity or low sensitivity.
MeSH Terms
Figure
-
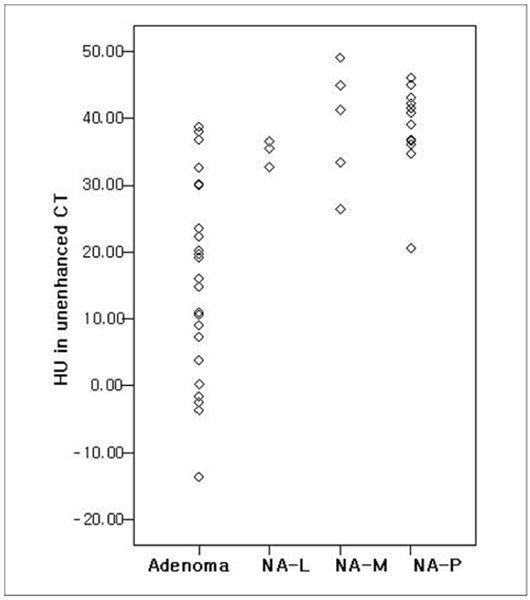
Fig. 1 Scattergram of the attenuation values in the unenhanced CT of 25 adenomas and each group of 20 nonadenomas (NA-L: lymphoma, NA-M: metastasis, NA-P: pheochromocytoma). Note that all masses with a HU < 20 were adenomas. Among the 20 nonadenomas, none had an attenuation value < 20, and eighteen (90%) of the nonadenomas had attenuation values > 30 HU.
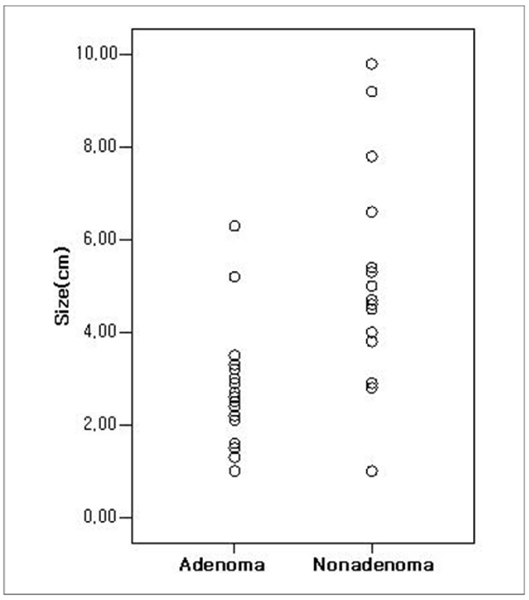
Fig. 2 Scattergram of the adenomas and nonadenomas according to their size.
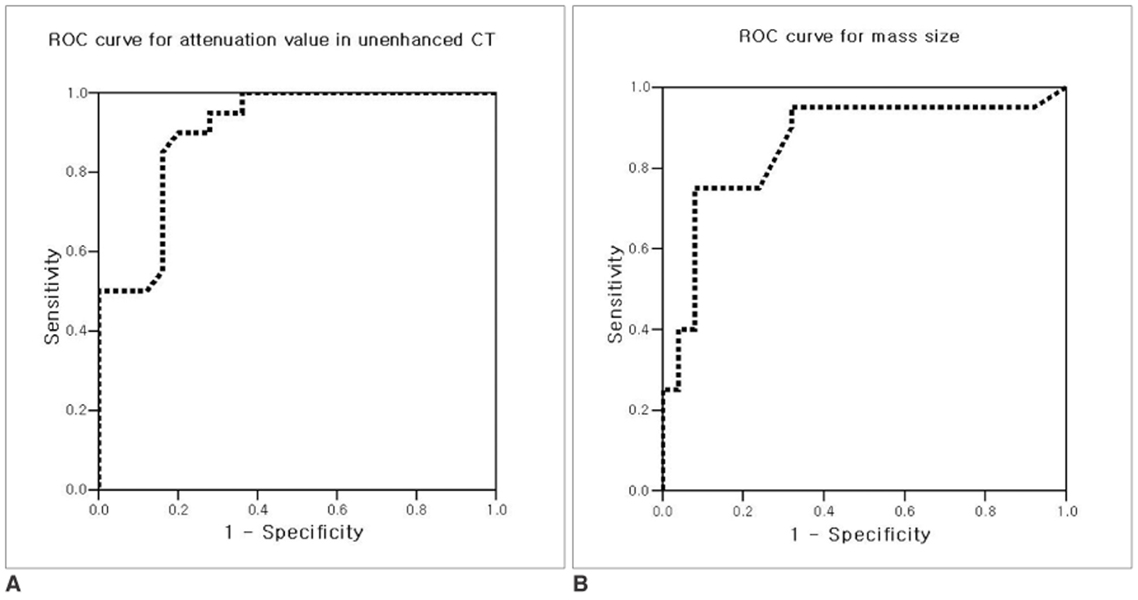
Fig. 3 Receiver operating characteristic curve for unenhanced CT attenuation value in enabling differentiation of adenomas from nonadenomas (A) and receiver operating characteristic curve for the size of adrenal lesions (B). The area under the receiver operating characteristic curve for CT attenuation values (0.904±0.044) was larger than that for size (0.860±0.060), indicating a greater ability of unenhanced CT attenuation value for distinguishing adenomas from nonadenomas.
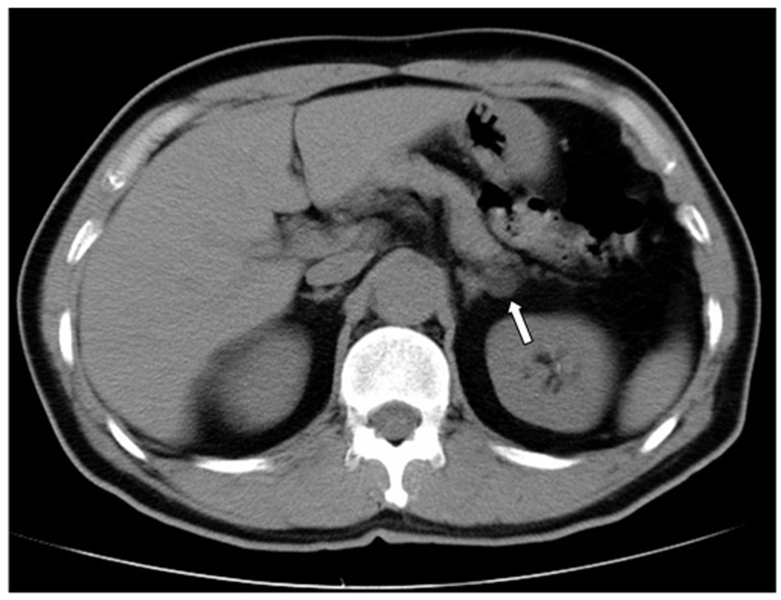
Fig. 4 Example of a typical adrenal adenoma in the noncontrast image. A 1.6 × 1.2 cm, well-defined, low attenuated nodule (arrow) is shown in the left adrenal gland with a HU value of -13.6. This nodule was confirmed to be an adrenal adenoma by a pathological examination.

Fig. 5 Non-contrast CT image of a 57 year-old female adrenal gland, showing a 2.9 × 2.7 cm, round-shaped nodule (arrow) in the left adrenal gland with a HU value of 38.7. The nodule was confirmed to be a benign adrenal adenoma by a pathological examination.

Fig. 6 Noncontrast abdominal CT scan of 17-year-old male, showing a 5.4 × 3.3 cm right adrenal mass (arrow) with a HU value of 33.4, which was suggestive of a nonadenoma rather than an adrenal adenoma. This mass was confirmed by a pathological examination to be a right adrenal metastasis from a renal cell carcinoma.
Reference
-
1. Kloos RT, Gross MD, Francis IR, Korobkin M, Shapiro B. Incidentally discovered adrenal masses. Endocr Rev. 1995. 16:460–484.2. Caplan RH, Strutt PJ, Wickus GG. Subclinical hormone secretion by incidentally discovered adrenal masses. Arch Surg. 1994. 129:291–296.3. Herrera MF, Grant CS, van Heerden JA, Sheedy PF, Ilstrup DM. Incidentally discovered adrenal tumors: an institutional perspective. Surgery. 1991. 110:1014–1021.4. Kokko JP, Brown TC, Berman MM. Adrenal adenoma and hypertension. Lancet. 1967. 1:468–470.5. Dobbie JW. Adrenocortical nodular hyperplasia: the ageing adrenal. J Pathol. 1969. 99:1–18.6. Abecassis M, McLoughlin MJ, Langer B, Kudlow JE. Serendipitous adrenal masses: prevalence, significance, and management. Am J Surg. 1985. 149:783–788.7. Oliver TW, Bernardino ME, Miller JI, Mansour K, Greene D, Davis WA. Isolated adrenal masses in nonsmall-cell bronchogenic carcinoma. Radiology. 1984. 153:217–218.8. Welch TJ, Sheedy PF 2nd, Stephens DH, Johnson CM, Swensen SJ. Percutaneous adrenal biopsy: review of a 10-year experience. Radiology. 1994. 193:341–344.9. Heaston DK, Handel DB, Ashton PR, Korobkin M. Narrow gauge needle aspiration of solid adrenal masses. AJR Am J Roentgenol. 1982. 138:1143–1148.10. Tang CK, Gray GF. Adrenocortical neoplasms. Prognosis and morphology. Urology. 1975. 5:691–695.11. Bernardino ME, Walther MM, Phillips VM, Graham SD Jr, Sewell CW, Gedgaudas-McClees K, et al. CT-guided adrenal biopsy: accuracy, safety, and indications. AJR Am J Roentgenol. 1985. 144:67–69.12. Korobkin M, Brodeur FJ, Yutzy GG, Francis IR, Quint LE, Dunnick NR, et al. Differentiation of adrenal adenomas from nonadenomas using CT attenuation values. AJR Am J Roentgenol. 1996. 166:531–536.13. Glazer HS, Weyman PJ, Sagel SS, Levitt RG, McClennan BL. Nonfunctioning adrenal masses: incidental discovery on computed tomography. AJR Am J Roentgenol. 1982. 139:81–85.14. Miyake H, Maeda H, Tashiro M, Suzuki K, Nagatomo H, Aikawa H, et al. CT of adrenal tumors: frequency and clinical significance of low-attenuation lesions. AJR Am J Roentgenol. 1989. 152:1005–1007.15. Lee MJ, Hahn PF, Papanicolaou N, Egglin TK, Saini S, Mueller PR, et al. Benign and malignant adrenal masses: CT distinction with attenuation coefficients, size, and observer analysis. Radiology. 1991. 179:415–418.16. van Erkel AR, van Gils AP, Lequin M, Kruitwagen C, Bloem JL, Falke TH. CT and MR distinction of adenomas and nonadenomas of the adrenal gland. J Comput Assist Tomogr. 1994. 18:432–438.17. Singer AA, Obuchowski NA, Einstein DM, Paushter DM. Metastasis or adenoma? Computed tomographic evaluation of the adrenal mass. Cleve Clin J Med. 1994. 61:200–205.18. Korobkin M, Giordano TJ, Brodeur FJ, Francis IR, Siegelman ES, Quint LE, et al. Adrenal adenomas: relationship between histologic lipid and CT and MR findings. Radiology. 1996. 200:743–747.19. Miyake H, Takaki H, Matsumoto S, Yoshida S, Maeda T, Mori H. Adrenal nonhyperfunctioning adenoma and nonadenoma: CT attenuation value as discriminative index. Abdom Imaging. 1995. 20:559–562.20. McNicholas MM, Lee MJ, Mayo-Smith WW, Hahn PF, Boland GW, Mueller PR. An imaging algorithm for the differential diagnosis of adrenal adenomas and metastases. AJR Am J Roentgenol. 1995. 165:1453–1459.21. Boland GW, Lee MJ, Gazelle GS, Halpern EF, McNicholas MM, Mueller PR. Characterization of adrenal masses using unenhanced CT: an analysis of the CT literature. AJR Am J Roentgenol. 1998. 171:201–204.22. Korobkin M, Brodeur FJ, Francis IR, Quint LE, Dunnick NR, Londy F. CT time-attenuation washout curves of adrenal adenomas and nonadenomas. AJR Am J Roentgenol. 1998. 170:747–752.23. Bertherat J, Mosnier-Pudar H, Bertagna X. Adrenal incidentalomas. Curr Opin Oncol. 2002. 14:58–63.24. Grumbach MM, Biller BM, Braunstein GD, Campbell KK, Carney JA, Godley PA, et al. Management of the clinically inapparent adrenal mass ("incidentaloma"). Ann Intern Med. 2003. 138:424–429.25. Nwariaku FE, Champine J, Kim LT, Burkey S, O'Keefe G, Snyder WH. Radiologic characterization of adrenal masses: the role of computed tomography-derived attenuation values. Surgery. 2001. 130:1068–1071.26. Leroy-Willig A, Roucayrol JC, Luton JP, Courtieu J, Niesenbaum N, Louvel A. In vitro adrenal cortex lesions characterization by NMR spectroscopy. Magn Reson Imaging. 1987. 5:339–344.27. Leroy-Willig A, Bittoun J, Luton JP, Louvel A, Lefevre JE, Bonnin A, et al. In vivo MR spectroscopic imaging of the adrenal glands: distinction between adenomas and carcinomas larger than 15 mm based on lipid content. AJR Am J Roentgenol. 1989. 153:771–773.28. Päivänsalo M, Lähde S, Merikanto J, Kallionen M. Computed tomography in primary and secondary adrenal tumours. Acta Radiol. 1988. 29:519–522.29. Szolar DH, Kammerhuber FH. Adrenal adenomas and nonadenomas: assessment of washout at delayed contrast-enhanced CT. Radiology. 1998. 207:369–375.30. Caoili EM, Korobkin M, Francis IR, Cohan RH, Platt JF, Dunnick NR, et al. Adrenal masses: characterization with combined unenhanced and delayed enhanced CT. Radiology. 2002. 222:629–633.31. Mayo-Smith WW, Boland GW, Noto RB, Lee MJ. State-of-the-art adrenal imaging. Radiographics. 2001. 21:995–1012.32. Hussain S, Belldegrun A, Seltzer SE, Richie JP, Gittes RF, Abrams HL. Differentiation of malignant from benign adrenal masses: predictive indices on computed tomography. AJR Am J Roentgenol. 1985. 144:61–65.33. Copeland PM. The incidentally discovered adrenal mass. Ann Intern Med. 1983. 98:940–945.34. Korobkin M, Francis IR, Kloos RT, Dunnick NR. The incidental adrenal mass. Radiol Clin North Am. 1996. 34:1037–1054.35. Mitnick JS, Bosniak MA, Megibow AJ, Naidich DP. Nonfunctioning adrenal adenomas discovered incidentally on computed tomography. Radiology. 1983. 148:495–499.36. Hamrahian AH, Ioachimescu AG, Remer EM, Motta-Ramirez G, Bogabathina H, Levin HS, et al. Clinical utility of noncontrast computed tomography attenuation value (hounsfield units) to differentiate adrenal adenomas/hyperplasias from nonadenomas: Cleveland Clinic experience. J Clin Endocrinol Metab. 2005. 90:871–877.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of Percentage Enhancement Washout Value Calculated on Unenhanced, Contrast-Enhanced, and Delayed Enhanced CT in Adrenal Masses: Adenoma versus Metastasis
- Detection of Acute Intraventricular Hemorrhage: Comparison of FLAIR MR Imaging with Unenhanced CT
- A case of idiopathic hyperaldosteronism vs. bilateral aldosterone producing adenoma
- CT diagnosis of adrenal disease
- A 5-Year Prospective Follow-Up Study of Lipid-Rich Adrenal Incidentalomas: No Tumor Growth or Development of Hormonal Hypersecretion
