Endovascular Management of Immediate Procedure-Related Complications of Failed Hemodialysis Access Recanalization
- Affiliations
-
- 1Department of Radiology, Chosun University Hospital, Korea. dhk1107@hanmail.net
- 2Department of Radiology, Soonchunhyang University Hospital, Korea.
- 3Department of General Surgery, Soonchunhyang University Hospital, Korea.
- KMID: 1102716
- DOI: http://doi.org/10.3348/kjr.2005.6.3.185
Abstract
- Endovascular procedures are becoming the standard type of care for the management of hemodialysis vascular access dysfunction. As with any type of medical procedure, these techniques can result in procedure-related complications, although the expected number of complications is low. The clinical extent of these complications varies from case to case. Management of these cases depends on the clinical presentation. Major complications such as vein rupture, arterial embolism, remote site bleeding or hematoma, symptomatic pulmonary embolism and puncture site complications necessitating treatment require major therapy. Minor complications such as non-flow compromising small puncture site hematoma or pseudoaneurysms require little or no therapy. It is essential that the interventionist be prepared to manage these complications appropriately when they arise.
Keyword
MeSH Terms
Figure
-

Fig. 1 58-year-old woman with a left radiocephalic fistula. A. Diffuse stenosis of the distal cephalic vein is shown. B. Contrast extravasation after ballooning is shown at the proximal diffuse stenotic lesion. C. Blood flow is blocked by a balloon catheter for five minutes. D. Postprocedural angiography shows restoration of the lumen.
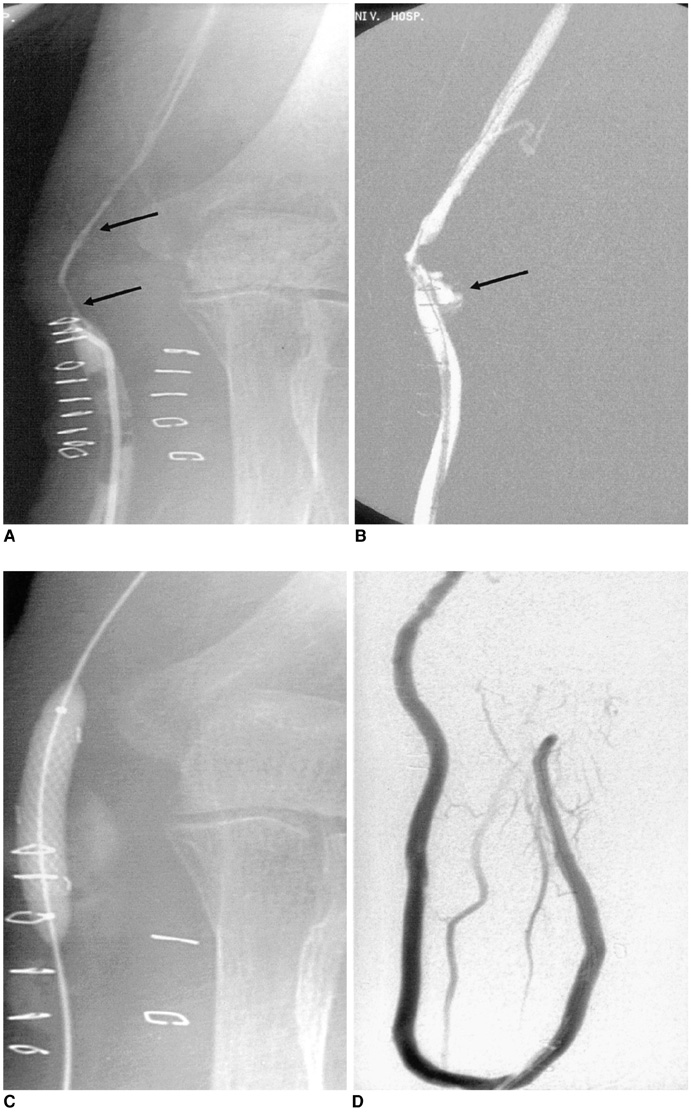
Fig. 2 47-year-old woman with a left radiobasilic graft. A. Diffuse tight stenosis is shown at the venous anastomosis (arrows). B. Extravasation after ballooning causing vein rupture. C. Blood flow was blocked by a balloon catheter for five minutes. However, fistulography shows continuous extravasation and persistent residual stenosis by severe tears and ruptures of the vein. Endovascular stents were successfully used to stop the bleeding and preserve the access. D. Follow-up angiography shows good patency of the lumen and no leakage.

Fig. 3 68-year-old woman with a right upper arm brachiobasilic graft. A. Abrupt cutoff in the ulnar artery means an arterial embolus. B. 7F Desilet-Hoffman sheath was advanced through the artery near the embolus. C. Angiography after retraction of the embolus in the sheath demonstrates a successful retrieval resulting in the restoration of the arterial lumen. D. The retracted embolus is shown.
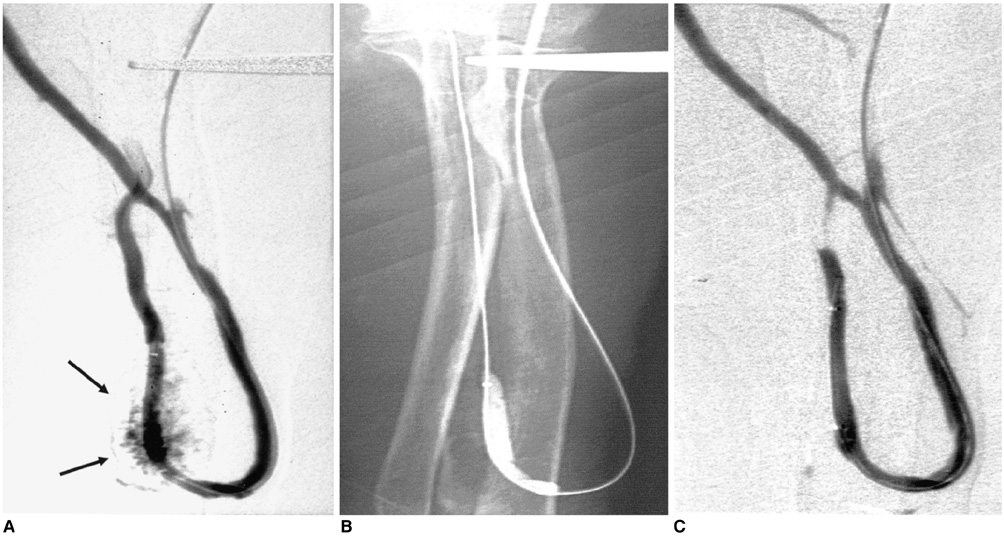
Fig. 4 55-year-old man with a left radiocephalic fistula. A. Extravasation from the distal radial artery is shown. B. Blood flow is blocked by an angioplasty balloon for five minutes. C. A follow-up angiography shows no blood leaking. There are no hemodynamically significant complications.
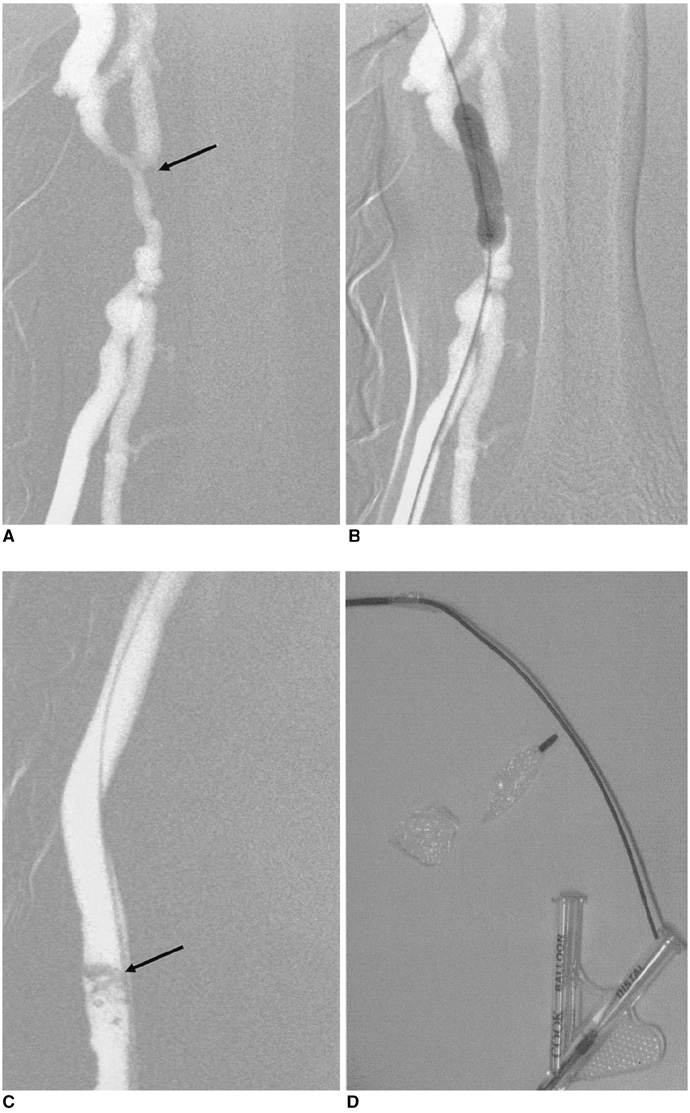
Fig. 5 56-year-old woman with a left upper arm brachiobrachial graft. A. Tight stenosis at the venous anastomosis (arrow). B. An angioplasty was attempted, but the balloon ruptured abruptly. C. Fragmented balloon is shown in contrast filled vascular lumen. The fragmented balloon was removed by open surgery. D. Fragmented balloon specimen, removed.

Fig. 6 48-year-old woman with a right upper arm brachiojugular graft. A. Intragraft filling defects means thrombi (arrows). B. Thrombi aspiration with Desilets-Hoffman sheath was performed. During the procedure the patient experienced chest discomfort and dyspnea. The final fistulography shows no abnormal filling defect. C. Perfusion defect is shown in upper left lobe. The patient was managed by conservative treatment with anticoagulant.
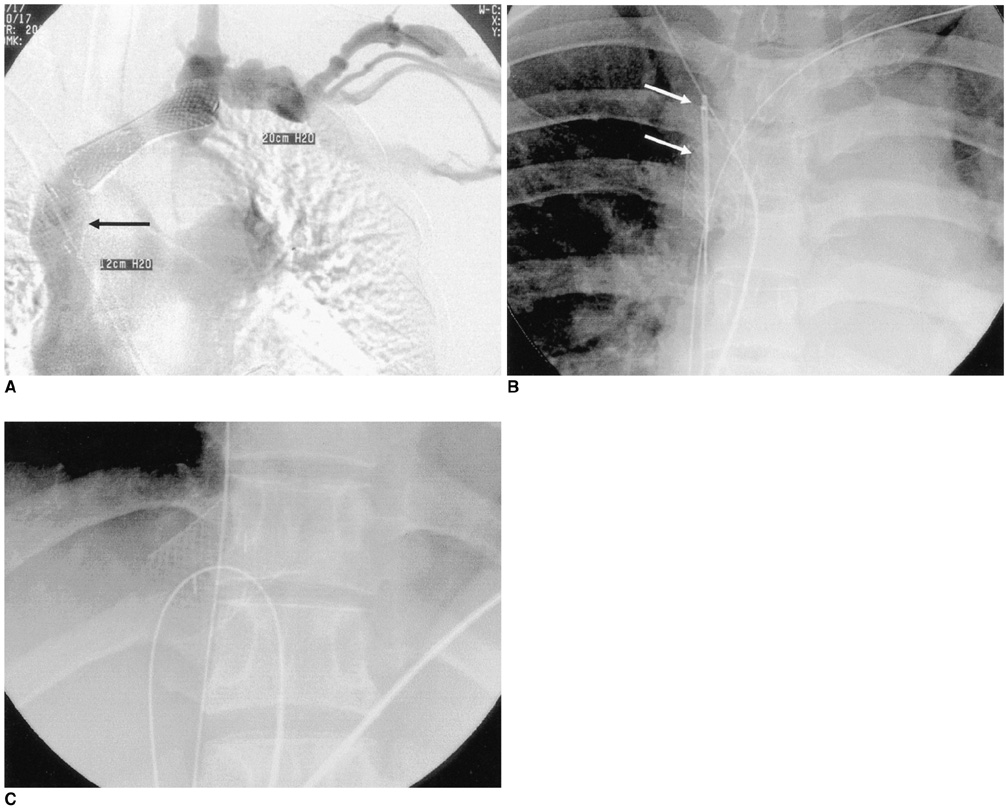
Fig. 7 29-year-old woman with a left upper arm brachiocephalic fistula. A. 20×20 mm-stent migration into superior vena cava is shown (arrow). B. 6F-Goose neck snare (arrows) and 5 F-catheter were inserted into SVC (displaced stent) via a 12 F-sheath of the femoral vein. C. Guide wire through the 5 F-catheter was snared. The displaced stent, "Wire-loop" made by pulled Goose neck snare and guide wire is removed via the femoral vein sheath.
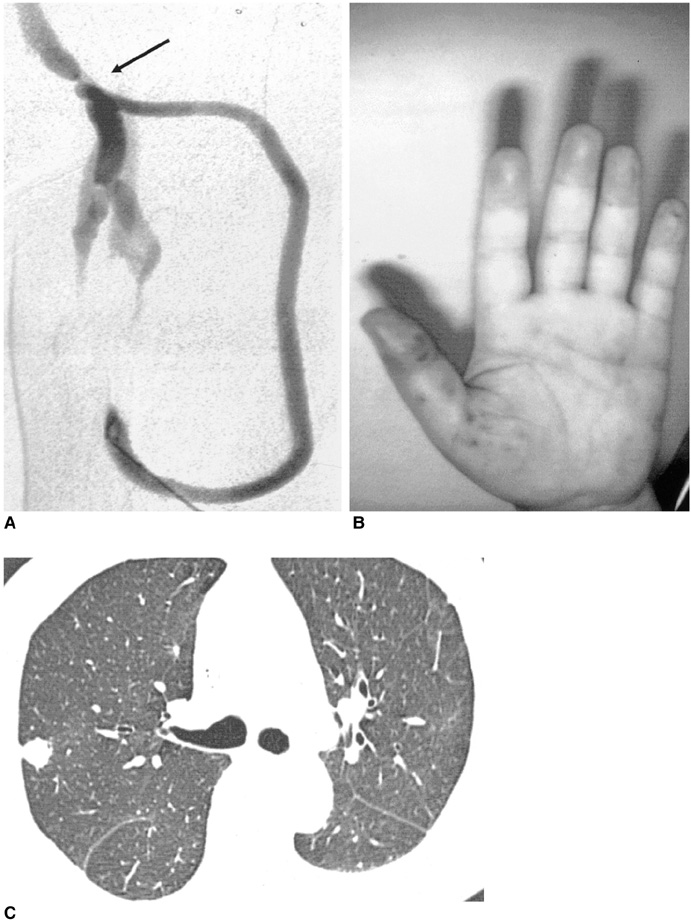
Fig. 8 63-year-old man with an infected graft and stenosis of the venous anastomosis. A. The patient had a focal infection in the arterial limb of the graft. Angiography shows focal stenosis at the venous anastomosis (arrow). B. Angioplasty was performed successfully. After one day, the patient experienced high fever and petechiae in the phalanges. C. After two weeks, multiple nodules were seen in the periphery of both lung fields. Yersinia Enterocolitica was confirmed microbiologically in pleural effusion and blood.
Reference
-
1. Sacks D, Marinelli DL, Martin LG, Spies JB. Society of Interventional Radiology Technology Assessment Committee. Reporting standards for clinical evaluation of new peripheral arterial revascularization devices. J Vasc Interv Radiol. 2003. 14(9Pt2):S395–S404.2. Sullivan KL, Besarab A, Bonn J, Shapiro MJ, Gardiner GA Jr, Moritz MJ. Hemodynamics of failing dialysis grafts. Radiology. 1993. 186:867–872.3. Weng FL, Berns JS. Complications of percutaneous treatment of thrombosed hemodialysis access grafts. Semin Dial. 2003. 16:257–262.4. Sofocleous CT, Schur I, Koh E, Hinrichs C, Cooper SG, Welber A, et al. Percutaneous treatment of complications occurring during hemodialysis graft recanalization. Eur J Radiol. 2003. 47:237–246.5. Trerotola SO, Lund GB, Scheel PJ Jr, Savader SJ, Venbrux AC, Osterman FA Jr. Thrombosed dialysis access grafts: percutaneous mechanical declotting without urokinase. Radiology. 1994. 191:721–726.6. Valji K, Bookstein JJ, Roberts AC, Davis GB. Pharmacomechanical thrombolysis and angioplasty in the management of clotted hemodialysis grafts: early and late clinical results. Radiology. 1991. 178:243–247.7. Beathard GA. Percutaneous transvenous angioplasty in the treatment of vascular access stenosis. Kidney Int. 1992. 42:1390–1397.8. Turmel-Rodriguez L, Pengloan J, Blanchier D, et al. Insufficient dialysis shunts: improved long-term patency rates with close hemodynamic monitoring, repeated percutaneous balloon angioplasty and stent placement. Radiology. 1993. 187:273–278.9. Beathard GA. Angioplasty for arteriovenous grafts and fistulae. Semin Nephrol. 2002. 22:202–210.10. Rundback JH, Leonardo RF, Poplausky MR, Rozenblit G. Venous rupture complicating hemodialysis access angioplasty: percutaneous treatment and outcomes in seven patients. AJR Am J Roentgenol. 1998. 171:1081–1084.11. Funaki B, Szymski GX, Leef JA, Rosenblum JD, Burke R, Hackworth CA. Wallstent deployment to salvage dialysis graft thrombolysis complicated by venous rupture: early and intermediate results. AJR Am J Roentgenol. 1997. 169:1435–1437.12. Beathard GA, Welch BR, Maidment HJ. Mechanical thrombolysis for the treatment of thrombosed hemodialysis access grafts. Radiology. 1996. 200:711–716.13. Trerotola SO, Johnson MS, Shah H, Namyslowski J. Backbleeding technique for treatment of arterial emboli resulting from dialysis graft thrombolysis. J Vasc Interv Radiol. 1998. 9(1Pt1):141–143.14. Cohen MA, Kumpe DA, Durham JD, Zwerdlinger SC. Improved treatment of thrombosed hemodialysis access sites with thrombolysis and angioplasty. Kidney Int. 1994. 46:1375–1380.15. Slonim SM, Dake MD, Razavi MK, Kee ST, Samuels SL, Rhee JS, et al. Management of misplaced or migrated endovascular stents. J Vasc Interv Radiol. 1999. 10:851–859.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Therapy to Salvage Hemodialysis Access
- Proximal Vein Obstruction or Stenosis Failed to Angioplasty in Hemodialysis Patients: Treatment with Endovascular Stent
- Endovascular Management for Malfunctioning Hemodialysis Access
- Clinical Experience with a Hybrid Procedure Using the Adherent Clot Catheter for Salvage of Thrombosed Hemodialysis Access: A Comparison with the Standard Fogarty Balloon Catheter
- Endovascular interventions for central vein stenosis
