Inflammatory Myofibroblastic Tumor: a Possible Complication of Percutaneous Radiofrequency Ablation for Hepatocellular Carcinoma
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Korea.
- 2Institute of Radiation Medicine, Seoul National University Hospital, Korea.shkim@radcom.snu.ac.kr
- 3Department of Pathology, Seoul National University Hospital, Korea.
- KMID: 1102568
- DOI: http://doi.org/10.3348/kjr.2009.10.6.635
Abstract
- An inflammatory myofibroblastic tumor (IMT) is an uncommon, benign lesion characterized by the mesenchymal proliferation and infiltration of inflammatory cells composed primarily of lymphocytes and plasma cells. A percutaneous radiofrequency ablation (RFA) is an effective and safe therapeutic modality used for the management of liver malignancies. Here we report, for the first time, a case of IMT as a complication of RFA for hepatocellular carcinoma in a 61-year-old man with a Child's class A hepatitis B-related liver cirrhosis. Gastrohepatic fistula formation was pathologically proven and associated with the RFA. Such a longstanding inflammation of the fistula might have been a possible cause of the development of IMT in this case.
MeSH Terms
Figure
-
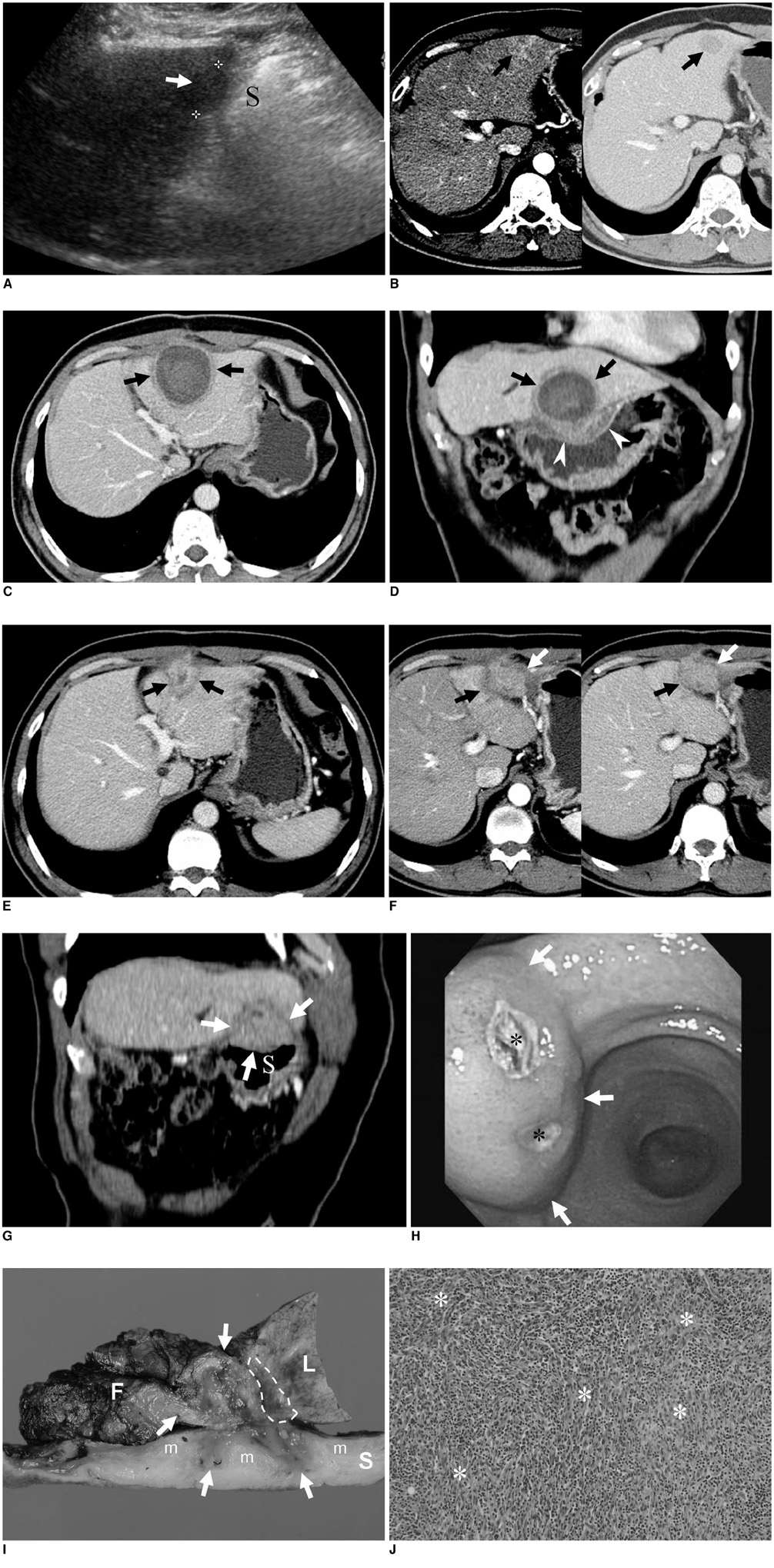
Fig. 1 61-year-old man with 2.3 cm-sized hepatocellular carcinoma in segment III of liver. A. On sagittal US image, low echoic nodule (arrow) is seen in left lateral segment of liver. Note proximity of lesion to stomach (S). B. Contrast-enhanced CT images display well-demarcated lesion (arrows) showing subtle enhancement on arterial phase (left) and washout of contrast material on portal venous phase (right). C, D. Axial (C) and coronal reformatted (D) CT image obtained one month after radiofrequency ablation revealing thick-walled cyst-like appearance (arrows) of radiofrequency ablation site. Asymmetric and heterogeneously enhancing wall thickening (arrowheads in D) suggesting thermal injury is noted at adjacent lesser curvature of stomach. 61-year-old man with 2.3 cm-sized hepatocellular carcinoma in segment III of liver. E-G. Follow-up portal phase CT image (E) obtained three months after radiofrequency ablation shows collapse (arrows) of previously seen, thick-walled, cystic lesion at radiofrequency ablation site. However, arterial (left in F) and portal (right in F) phase CT scans obtained 2.5 cm below (E) demonstrate ill-defined mass (arrows) with thick and irregular low attenuating rim. This lesion shows slight hyperattenuation on arterial phase (left in F) and slight low attenuation on portal venous (right in F) phase. Therefore, at time of interpretation, tentative radiologic diagnosis was marginal recurrence of hepatocellular carcinoma. Coronal reformatted CT image (G) obtained during portal venous phase displays mass (arrows) extending exophytically and to extrahepatic portion of mass, which was in contact with and compressing adjacent stomach (S). Gastroscopy (H) demonstrates 2.5 cm submucosal mass (arrows) at lesser curvature side of gastric angle. Two small ulcerations (*) observed at center of lesion. 61-year-old man with 2.3 cm-sized hepatocellular carcinoma in segment III of liver. I. Cut section of gross specimen obtained after performing hepatic tumorectomy and distal gastrectomy shows that mass (arrows) was mainly located in perihepatic fatty tissue (F) and extended to adjacent hepatic parenchyma (L) as well as proper muscle layer (m) of stomach (S). Area of coagulation necrosis (dotted line) induced by previous radiofrequency ablation was pushed upwards by mass. In addition, there were three openings of fistulous tract at mucosa of adherent stomach. Moreover, fistulous tract communicated with liver parenchyma (not shown). J. Upon microscopic examination (Hematoxylin & Eosin staining, ×100), elongated spindled myofibroblasts (*) were predominantly seen with heavy infiltration of lymphocytes and plasma cells. Inflammatory myofibroblastic tumor of compact spindle cell pattern was finally concluded as diagnosis.
Reference
-
1. Anthony PP, Telesinghe PU. Inflammatory pseudotumour of the liver. J Clin Pathol. 1986. 39:761–768.2. Lawrence B, Perez-Atayde A, Hibbard MK, Rubin BP, Dal Cin P, Pinkus JL, et al. TPM3-ALK and TPM4-ALK oncogenes in inflammatory myofibroblastic tumors. Am J Pathol. 2000. 157:377–384.3. Livraghi T, Goldberg SN, Lazzaroni S, Meloni F, Ierace T, Solbiati L, et al. Hepatocellular carcinoma: radio-frequency ablation of medium and large lesions. Radiology. 2000. 214:761–768.4. Rhim H, Yoon KH, Lee JM, Cho Y, Cho JS, Kim SH, et al. Major complications after radio-frequency thermal ablation of hepatic tumors: spectrum of imaging findings. Radiographics. 2003. 23:123–134.5. Bruix J, Sherman M. Practice Guidelines Committee. American Association for the Study of Liver Diseases. Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005. 42:1208–1236.6. Lee JM, Han JK, Kim HC, Choi YH, Kim SH, Choi JY, et al. Switching monopolar radiofrequency ablation technique using multiple, internally cooled electrodes and a multichannel generator: ex vivo and in vivo pilot study. Invest Radiol. 2007. 42:163–171.7. Akahane M, Koga H, Kato N, Yamada H, Uozumi K, Tateishi R, et al. Complications of percutaneous radiofrequency ablation for hepatocellular carcinoma: imaging spectrum and management. Radiographics. 2005. 25:S57–S68.8. Gleason BC, Hornick JL. Inflammatory myofibroblastic tumours: where are we now? J Clin Pathol. 2008. 61:428–437.9. Coffin CM, Watterson J, Priest JR, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor (inflammatory pseudotumor). A clinicopathologic and immunohistochemical study of 84 cases. Am J Surg Pathol. 1995. 19:859–872.10. Bessoud B, Doenz F, Qanadli SD, Nordback P, Schnyder P, Denys A. Enterobiliary fistula after radiofrequency ablation of liver metastases. J Vasc Interv Radiol. 2003. 14:1581–1584.11. Falco A, Orlando D, Sciarra R, Sergiacomo L. A case of biliary gastric fistula following percutaneous radiofrequency thermal ablation of hepatocellular carcinoma. World J Gastroenterol. 2007. 13:804–805.12. Kondo Y, Yoshida H, Shiina S, Tateishi R, Teratani T, Omata M. Artificial ascites technique for percutaneous radiofrequency ablation of liver cancer adjacent to the gastrointestinal tract. Br J Surg. 2006. 93:1277–1282.13. Kim HC, Lee JM, Kim KW, Park SH, Kim SH, Lee JY, et al. Gastrointestinal stromal tumors of the stomach: CT findings and prediction of malignancy. AJR Am J Roentgenol. 2004. 183:893–898.14. Lokken RP, Gervais DA, Arellano RS, Tuncali K, Morrison PR, Tatli S, et al. Inflammatory nodules mimic applicator track seeding after percutaneous ablation of renal tumors. AJR Am J Roentgenol. 2007. 189:845–848.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Small Bowel Perforation after Percutaneous Ultrasound-guided Radiofrequency Ablation of Hepatocellular Carcinoma
- Completely Ablated Hepatocellular Carcinoma by Percutaneous Radiofrequency Thermal Ablation
- Microwave thermosphere versus radiofrequency ablation for hepatocellular carcinoma: Are we approaching the time to end the debate?
- Chemoembolization combined with radiofrequency ablation is the best option for the local treatment of early hepatocellular carcinoma?
- Radiofrequency Ablation of Hepatic Cysts: Case Report
