Hepatocellular Carcinomas Smaller Than 4 cm Supplied by the Intercostal Artery: Can We Predict Which Intercostal Artery Supplies the Tumor?
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, Institute of Radiation Medicine, Seoul National University Medical Research Center, and Clinical Research Institute, Seoul National University Hospital, Seoul 110-744, Korea. angioint
- KMID: 1101923
- DOI: http://doi.org/10.3348/kjr.2011.12.6.693
Abstract
OBJECTIVE
To predict which intercostal artery supplies a tumor by examining the spatial relationship between hepatocellular carcinoma (HCC) and the intercostal artery feeding the tumor on transverse computed tomography (CT) images.
MATERIALS AND METHODS
Between January 2000 and September 2009, 46 intercostal arteries supplying HCCs smaller than 4 cm were noted in 44 patients, and CT scans and angiograms of these patients were retrospectively reviewed. The intercostal artery feeding the tumor was marked on the CT scan showing the center of the tumor. In addition, its spatial relationship with the tumor center was examined. The angle of the tumor location was measured on the transverse CT scan in the clockwise direction from the sagittal line on the virtual circle centered in the right hemithorax. Correlations between the angle of the tumor location and the level of the tumor-feeding intercostal artery were assessed with the Spearman rank coefficient.
RESULTS
Of 46 intercostal arteries feeding HCC, 39 (85%) were the first ones observed from the tumor center in a counterclockwise direction on the transverse CT image containing the tumor center. The level of the tumor-feeding intercostal artery was significantly correlated with the angle of the tumor, as the posteriorly located tumor tends to be supplied by lower intercostal arteries, while the laterally located tumor by upper intercostal arteries (Spearman coefficient = -0.537; p < 0.001).
CONCLUSION
We can predict the tumor feeder with an accuracy of 85% as the first intercostal artery encountered from the tumor center in a counterclockwise direction on a transverse CT image.
MeSH Terms
Figure
-

Fig. 1 Flowchart of study population enrollment with exclusion criteria. MDCT = multidetector CT

Fig. 2 68-year-old man with hepatocellular carcinoma who underwent 8 chemoembolization sessions. A. Transverse CT scan in hepatic arterial phase shows small hypervascular tumor (star). Center of virtual circle was drawn using following steps: 1) select CT transverse scan showing center of tumor, 2) horizontal line (-) inscribing posterior margin of thorax is drawn, 3) line is bisected by perpendicular line (=), which is again perpendicularly bisected by another horizontal line (≡); mid-point of line (≡) is defined as center of circle (arrowhead), concentric with hemithorax. B. Radial line passing through tumor center is drawn and its angle from sagittal line is measured as angle of tumor location (197 degrees in this case). Note 11th intercostal artery (arrow) below 11th rib. C. Selective angiography of 11th intercostal artery showing tumor staining (arrow) supplied by tumor feeder (arrowhead).
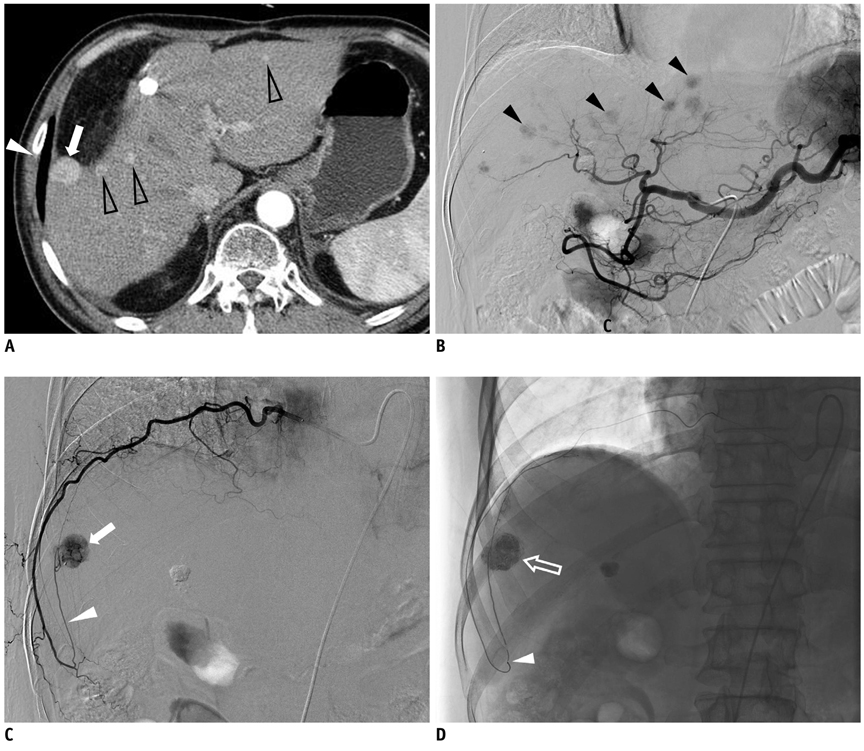
Fig. 3 61-year-old man with hepatocellular carcinoma who underwent 7 chemoembolization sessions. A. Transverse CT scan in hepatic arterial phase showing multiple small hypervascular tumors (arrow and open arrowheads). Note 9th intercostal artery below 9th rib. B. Celiac angiography performed during 8th chemoembolization session shows multiple small hypervascular tumor stainings (arrowheads) in liver. Tumor indicated by arrow in A is not evident on this celiac angiogram. C. Selective angiography of 9th intercostal artery shows tumor staining (arrow) supplied by tumor feeder (arrowhead), which makes sharp upward turn at costochondral junction. D. Spot image obtained during chemoembolization shows compact retention of iodized oil within tumor (arrow) and microcatheter tip (arrowhead) within tumor feeder.
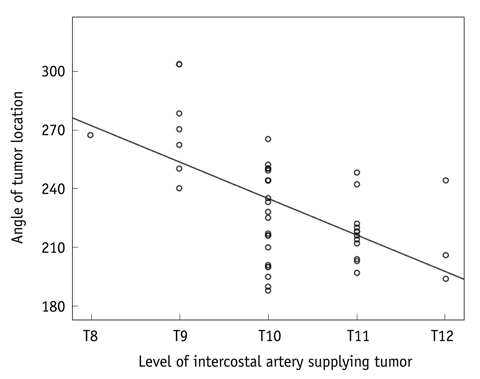
Fig. 4 Relationship between angle of tumor location and level of intercostal artery supplying tumor.
Reference
-
1. Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology. 2003. 37:429–442.2. Shin SW. The current practice of transarterial chemoembolization for the treatment of hepatocellular carcinoma. Korean J Radiol. 2009. 10:425–434.3. Lammer J, Malagari K, Vogl T, Pilleul F, Denys A, Watkinson A, et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc Intervent Radiol. 2010. 33:41–52.4. Ji SK, Cho YK, Ahn YS, Kim MY, Park YO, Kim JK, et al. Multivariate analysis of the predictors of survival for patients with hepatocellular carcinoma undergoing transarterial chemoembolization: focusing on superselective chemoembolization. Korean J Radiol. 2008. 9:534–540.5. Chung JW, Park JH, Han JK, Choi BI, Kim TK, Han MC. Transcatheter oily chemoembolization of the inferior phrenic artery in hepatocellular carcinoma: the safety and potential therapeutic role. J Vasc Interv Radiol. 1998. 9:495–500.6. Miyayama S, Matsui O, Nishida H, Yamamori S, Minami T, Shinmura R, et al. Transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma fed by the cystic artery. J Vasc Interv Radiol. 2003. 14:1155–1161.7. Kim HC, Chung JW, Lee W, Jae HJ, Park JH. Recognizing extrahepatic collateral vessels that supply hepatocellular carcinoma to avoid complications of transcatheter arterial chemoembolization. Radiographics. 2005. 25:Suppl 1. S25–S39.8. Park SI, Lee DY, Won JY, Lee JT. Extrahepatic collateral supply of hepatocellular carcinoma by the intercostal arteries. J Vasc Interv Radiol. 2003. 14:461–468.9. Suh SH, Won JY, Lee DY, Lee JT, Lee KH. Chemoembolization of the left inferior phrenic artery in patients with hepatocellular carcinoma: radiographic findings and clinical outcome. J Vasc Interv Radiol. 2005. 16:1741–1745.10. Wang YL, Li MH, Cheng YS, Shi HB, Fan HL. Influential factors and formation of extrahepatic collateral artery in unresectable hepatocellular carcinoma. World J Gastroenterol. 2005. 11:2637–2642.11. Chung JW, Kim HC, Yoon JH, Lee HS, Jae HJ, Lee W, et al. Transcatheter arterial chemoembolization of hepatocellular carcinoma: prevalence and causative factors of extrahepatic collateral arteries in 479 patients. Korean J Radiol. 2006. 7:257–266.12. Kim HC, Chung JW, Jae HJ, Lee W, So YH, Park JH. Hepatocellular carcinoma: transcatheter arterial chemoembolization of the gonadal artery. J Vasc Interv Radiol. 2006. 17:703–709.13. Miyayama S, Matsui O, Taki K, Minami T, Ryu Y, Ito C, et al. Extrahepatic blood supply to hepatocellular carcinoma: angiographic demonstration and transcatheter arterial chemoembolization. Cardiovasc Intervent Radiol. 2006. 29:39–48.14. Kim HC, Chung JW, Choi SH, Jae HJ, Lee W, Park JH. Internal mammary arteries supplying hepatocellular carcinoma: vascular anatomy at digital subtraction angiography in 97 patients. Radiology. 2007. 242:925–932.15. Kim HC, Chung JW, Choi SH, Yoon JH, Lee HS, Jae HJ, et al. Hepatocellular carcinoma with internal mammary artery supply: feasibility and efficacy of transarterial chemoembolization and factors affecting patient prognosis. J Vasc Interv Radiol. 2007. 18:611–619. quiz 620.16. Miyayama S, Yamashiro M, Okuda M, Yoshie Y, Sugimori N, Igarashi S, et al. Hepatocellular carcinoma supplied by the right lumbar artery. Cardiovasc Intervent Radiol. 2010. 33:53–60.17. Miyayama S, Yamashiro M, Okuda M, Yoshie Y, Nakashima Y, Ikeno H, et al. The march of extrahepatic collaterals: analysis of blood supply to hepatocellular carcinoma located in the bare area of the liver after chemoembolization. Cardiovasc Intervent Radiol. 2010. 33:513–522.18. Kim HC, Chung JW, An S, Seong NJ, Son KR, Jae HJ, et al. Transarterial chemoembolization of a colic branch of the superior mesenteric artery in patients with unresectable hepatocellular carcinoma. J Vasc Interv Radiol. 2011. 22:47–54.19. Kim HC, Chung JW, Lee IJ, An S, Seong NJ, Son KR, et al. Intercostal artery supplying hepatocellular carcinoma: demonstration of a tumor feeder by C-arm CT and multidetector row CT. Cardiovasc Intervent Radiol. 2011. 34:87–91.20. Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, et al. European Association for the Study of the Liver. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. J Hepatol. 2001. 35:421–430.21. Kim MW, Kim HC, Chung JW, An S, Seong NJ, Jae HJ. Hepatocellular carcinoma: prediction of blood supply from an intercostal artery with multi-detector row CT. J Vasc Interv Radiol. 2011. [Epub ahead of print].
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chemoembolization through Intercostal Arteries in Hepatocellular Carcinoma' Report of A Case of Transient Spinal Cord Injury
- Bifid Rib: Anatomical Considerations in Three Cases
- Transarterial Embolization of Acute Intercostal Artery Bleeding
- Refractory intercostal neuralgia due to intercostal schwannoma: A case report
- A case of spontaneous hemothorax associated with von Recklinghausen's disease
