Gastrointestinal Tract Perforation: MDCT Findings according to the Perforation Sites
- Affiliations
-
- 1Department of Radiology, Chonnam National University Hospital, Gwangju, Korea.
- 2Department of Radiology, Chonnam National University Medical School, Gwangju, Korea. kjradsss@dreamwiz.com
- 3Department of Radiology, Chonnam National University Hwasun Hospital, Jeollanam-do, Korea.
- KMID: 1088680
- DOI: http://doi.org/10.3348/kjr.2009.10.1.63
Abstract
- Our objective is to describe the characteristic CT findings of gastrointestinal (GI) tract perforations at various levels of the gastrointestinal system. It is beneficial to localize the perforation site as well as to diagnose the presence of bowel perforation for planning the correct surgery. CT has been established as the most valuable imaging technique for identifying the presence, site and cause of the GI tract perforation. The amount and location of extraluminal free air usually differ among various perforation sites. Further, CT findings such as discontinuity of the bowel wall and concentrated free air bubbles in close proximity to the bowel wall can help predict the perforation site. Multidetector CT with the multiplanar reformation images has improved the accuracy of CT for predicting the perforation sites.
Keyword
MeSH Terms
Figure
-
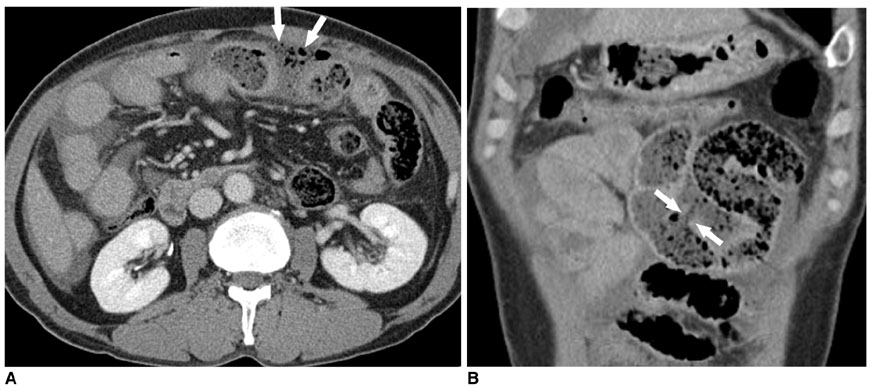
Fig. 1 46-year-old man with traumatic small bowel perforation. A. Transverse CT image shows concentrated free air bubbles (arrows) in vicinity of jejunal loop. B. Coronal reformation CT image demonstrates discontinuity of jejunal wall (arrows), which is not clearly seen on transverse CT image.

Fig. 2 47-year-old man with traumatic small bowel perforation. Transverse CT image shows small air bubble (arrow) at anterior abdominal surface. Presence of air is more clearly seen on CT image with wide window setting.

Fig. 3 Traumatic duodenal perforation in 53-year-old woman. Transverse CT scan demonstrates extraluminal free air (arrows) surrounding 3rd portion of duodenum (D) and retroperitoneal fluid (arrowheads).

Fig. 4 Pseudopneumoperitoneum in 53-year-old man. Transverse CT image shows free air bubbles (arrows) between transversalis fascia and parietal peritoneum, which could be misinterpreted as pneumoperitoneum.

Fig. 5 37-year-old woman with perforated gastric ulcer. Focal defect in lesser curvature of gastric body is caused by deep ulcer (arrow) associated with surrounding mural thickening. Note small air bubble (arrowhead) on anterior peritoneal surface of liver.
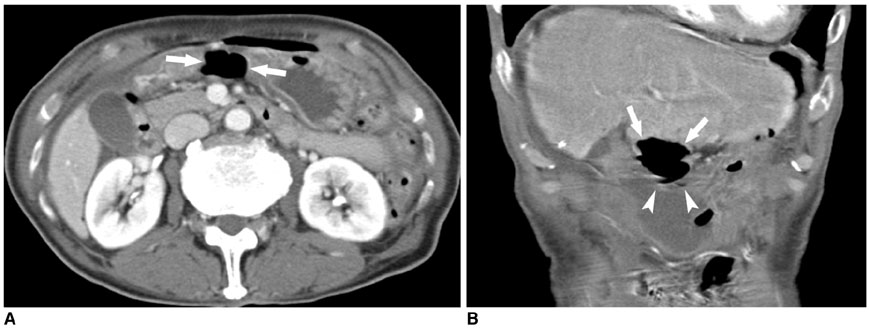
Fig. 6 74-year-old man with perforated gastric ulcer. A. Transverse CT image shows concentration of extraluminal air bubbles (arrows) in close proximity to gastric antral wall. B. Coronal reformation CT image demonstrates close relationship between extraluminal air bubbles (arrows) and gastric antral wall (arrowheads).
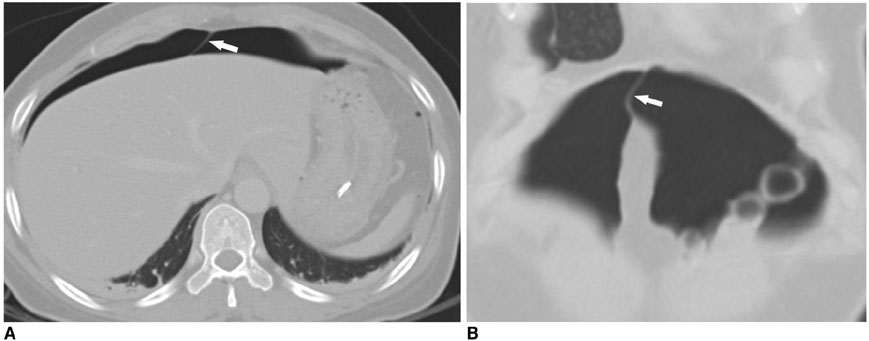
Fig. 7 41-year-old woman with perforation of gastric body that complicates endoscopic submucosal dissection. Transverse (A) and coronal reformation (B) CT images with wide window setting show that free air crossing midline accentuates falciform ligament (arrow).

Fig. 8 68-year-old woman with perforation of posterior wall of gastric body and this complicates endoscopic submucosal dissection. Transverse CT image shows free air (arrow) in lesser sac. Large quantity of free air (arrowheads) anterior to stomach is also seen.

Fig. 9 47-year-old man with small bowel perforation due to blunt trauma. Transverse CT image shows tiny air bubble (arrowhead) around perforated small bowel with thick enhancing wall (arrows).
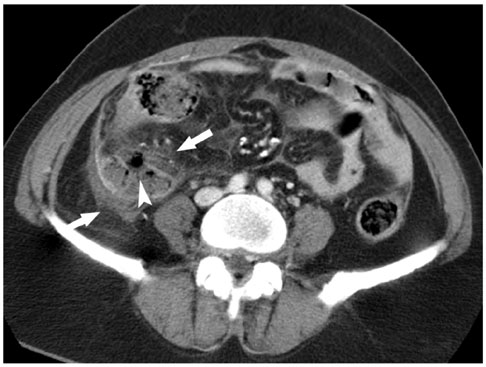
Fig. 10 49-year-old woman with acute perforated appendicitis. Transverse CT image demonstrates focal defect (arrowhead) in inflamed appendiceal wall and periappendiceal inflammatory stranding (arrows).

Fig. 11 74-year-old man with perforation of sigmoid colon. Transverse CT image shows extraluminal air-fluid level (arrows) adjacent to sigmoid colon with mural thickening and enhancement (arrowheads).
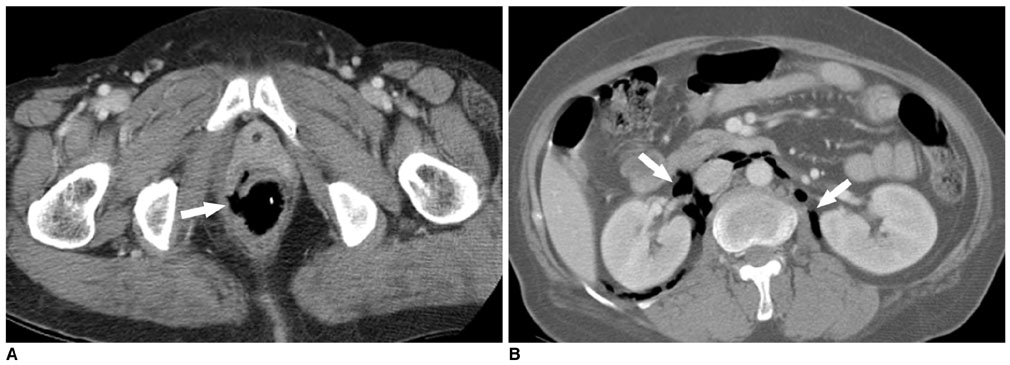
Fig. 12 60-year-old woman with iatrogenic rectal perforation. A. Transverse CT image shows focal defect (arrow) in right side of rectal wall. B. Transverse CT image demonstrates free air (arrows) in both perirenal spaces.
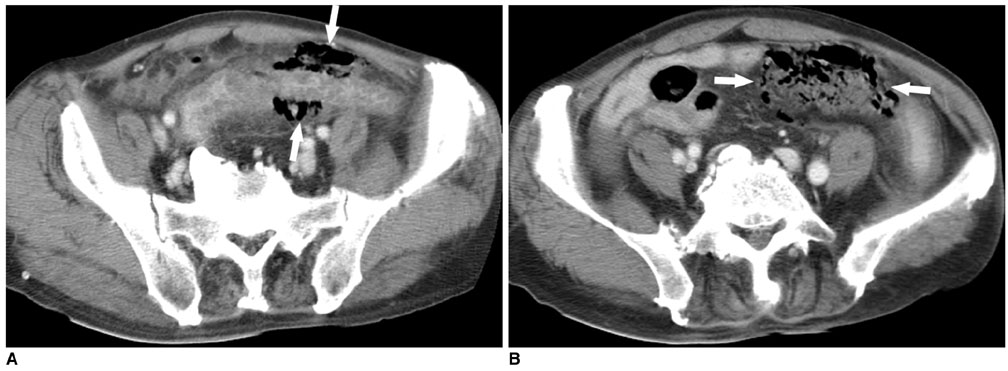
Fig. 13 81-year-old man with spontaneous perforation of sigmoid colon. A. Transverse CT image shows concentration of extraluminal air bubbles (arrows) in close proximity to sigmoid wall. B. Transverse CT image obtained at upper level demonstrates extraluminal feces, which display unique appearance of mass with mottled air bubbles (arrows).
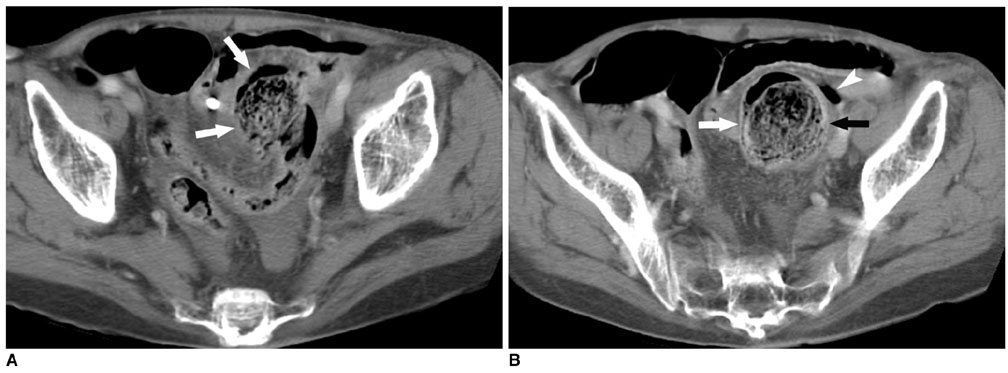
Fig. 14 90-year-old man with stercoral perforation of sigmoid colon. A. Transverse CT image shows localized hard fecal mass (arrows) connected with sigmoid colon. B. Transverse CT image obtained at upper level demonstrates extraluminal gas (arrowhead) adjacent to localized hard fecal mass (arrows), which is indicative of perforation.
Cited by 1 articles
-
Clinical Analysis of Stercoral Perforation of the Colon
Jung Kwang Nam, Byung Seok Kim, Kyung Soo Kim, Duk Jin Moon
Korean J Gastroenterol. 2010;55(1):46-51. doi: 10.4166/kjg.2010.55.1.46.
Reference
-
1. Yeung KW, Chang MS, Hsiao CP, Huang JF. CT evaluation of gastrointestinal tract perforation. Clin Imaging. 2004. 28:329–333.2. Siu WT, Chau CH, Law BK, Tang CN, Ha PY, Li MK. Routine use of laparoscopic repair for perforated peptic ulcer. Br J Surg. 2004. 91:481–484.3. Hainaux B, Agneessens E, Bertinotti R, De Maertelaer V, Rubesova E, Capelluto E, et al. Accuracy of MDCT in predicting site of gastrointestinal tract perforation. AJR Am J Roentgenol. 2006. 187:1179–1183.4. Donovan AJ, Berne TV, Donovan JA. Perforated duodenal ulcer: an alternative therapeutic plan. Arch Surg. 1998. 133:1166–1171.5. Furukawa A, Sakoda M, Yamasaki M, Kono N, Tanaka T, Nitta N, et al. Gastrointestinal tract perforation: CT diagnosis of presence, site, and cause. Abdom Imaging. 2005. 30:524–534.6. Ghekiere O, Lesnik A, Hoa D, Laffargue G, Uriot C, Taourel P. Value of computed tomography in the diagnosis of the cause of nontraumatic gastrointestinal tract perforation. J Comput Assist Tomogr. 2007. 31:169–176.7. Miki T, Ogata S, Uto M, Nakazono T, Urata M, Ishibe R, et al. Multidetector-row CT findings of colonic perforation: direct visualization of ruptured colonic wall. Abdom Imaging. 2004. 29:658–662.8. Brofman N, Atri M, Hanson JM, Grinblat L, Chughtai T, Brenneman F. Evaluation of bowel and mesenteric blunt trauma with multidetector CT. Radiographics. 2006. 26:1119–1131.9. Maniatis V, Chryssikopoulos H, Roussakis A, Kalamara C, Kavadias S, Papadopoulos A, et al. Perforation of the alimentary tract: evaluation with computed tomography. Abdom Imaging. 2000. 25:373–379.10. Imuta M, Awai K, Nakayama Y, Murata Y, Asao C, Matsukawa T, et al. Multidetector CT findings suggesting a perforation site in the gastrointestinal tract: analysis in surgically confirmed 155 patients. Radiat Med. 2007. 25:113–118.11. Kim HC, Shin HC, Park SJ, Park SI, Kim HH, Bae WK, et al. Traumatic bowel perforation: analysis of CT findings according to the perforation site and the elapsed time since accident. Clin Imaging. 2004. 28:334–339.12. Stuhlfaut JW, Soto JA, Lucey BC, Ulrich A, Rathlev NK, Burke PA, et al. Blunt abdominal trauma: performance of CT without oral contrast material. Radiology. 2004. 233:689–694.13. Meyers M. Meyers MA, editor. The extraperitoneal spaces: normal and pathologic anatomy. Dynamic radiology of the abdomen. 2000. 5th ed. New York: Springer-Verlag;333–492.14. Grassi R, Romano S, Pinto A, Romano L. Gastro-duodenal perforations: conventional plain film, US and CT findings in 166 consecutive patients. Eur J Radiol. 2004. 50:30–36.15. Kunin JR, Korobkin M, Ellis JH, Francis IR, Kane NM, Siegel SE. Duodenal injuries caused by blunt abdominal trauma: value of CT in differentiating perforation from hematoma. AJR Am J Roentgenol. 1993. 160:1221–1223.16. Grassi R, Pinto A, Rossi G, Rotondo A. Conventional plain-film radiology, ultrasonography and CT in jejuno-ileal perforation. Acta Radiol. 1998. 39:52–56.17. Birnbaum BA, Wilson SR. Appendicitis at the millennium. Radiology. 2000. 215:337–348.18. Horrow MM, White DS, Horrow JC. Differentiation of perforated from nonperforated appendicitis at CT. Radiology. 2003. 227:46–51.19. Ghahremani GG. Radiologic evaluation of suspected gastrointestinal perforations. Radiol Clin North Am. 1993. 31:1219–1234.20. Rozenblit AM, Cohen-Schwartz D, Wolf EL, Foxx MJ, Brenner S. Case reports. Stercoral perforation of the sigmoid colon: computed tomography findings. Clin Radiol. 2000. 55:727–729.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Neonatal Gastrointestinal Perforation
- Ileal Perforation due to Cytomegalovirus Infection in a Patient with Acquired Immunodeficiency Syndrome
- An unusual cause of duodenal perforation due to a lollipop stick
- Endoscopic closure of duodenal perforation using an endoloop anchored by hemoclips
- Spontaneous Perforation of Meckel's Diverticulum in a Neonate
