Eccrine Spiradenoma Arising in the Breast Misdiagnosed as an Epidermal Inclusion Cyst
- Affiliations
-
- 1Department of Radiology, Gachon University Gil Hospital, Incheon 405-760, Korea. shpark@gilhospital.com
- 2Department of Surgery, Gachon University Gil Hospital, Incheon 405-760, Korea.
- KMID: 1088573
- DOI: http://doi.org/10.3348/kjr.2011.12.2.256
Abstract
- Eccrine spiradenomas are rare, benign, cutaneous tumors that originate in the sweat glands. Eccrine spiradenomas in the breast are very rare and only a few cases have been reported. We report here on the case of a 47-year-old woman with superficial masses in the breast and these masses had gradually increased in size during follow-up. They were confirmed to be an eccrine spiradenoma on pathologic examination. There have been a few reports about the radiologic findings of eccrine spiradenomas of the breast. This is the first case of an eccrine spiradenoma in the breast that was characterized by multiple imaging modalities, including mammography, ultrasonography and MRI. The lesion in our patient was first diagnosed as an epidermal inclusion cyst based on the imaging findings and the mass's superficial location. Although the mammographic and ultrasonographic imaging findings of eccrine spiradenomas and epidermal inclusion cysts are similar, the MRI findings are different between epidermal inclusion cysts and eccrine spiradenomas. Eccrine spiradenomas should be considered in the differential diagnosis of cutaneous and subcutaneous lesions of the breast.
MeSH Terms
Figure
-
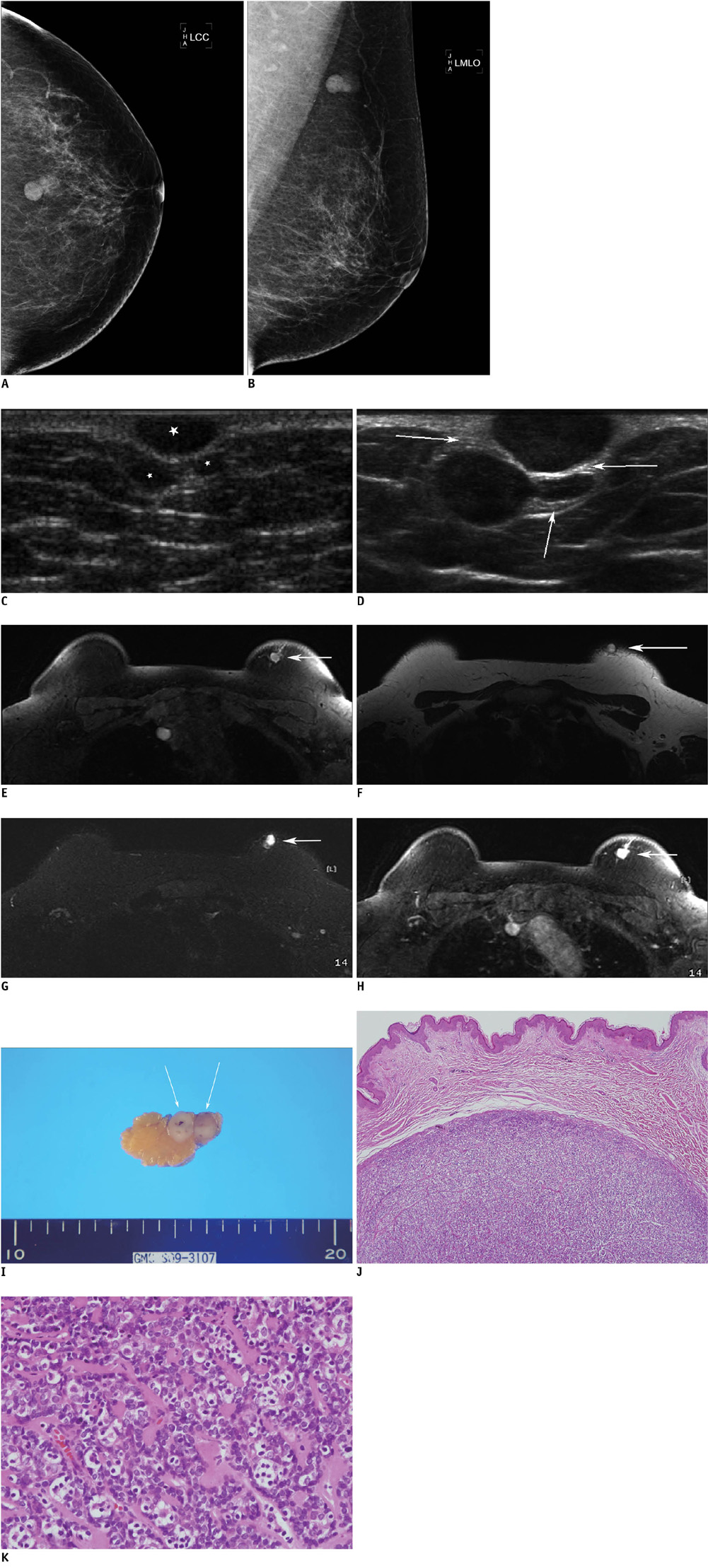
Fig. 1 Eccrine spiradenoma arising in breast in 47-year-old woman. A, B. Routine mammography was performed and this showed two well-defined nodular densities in left upper central quadrant. C, D. Breast US was performed on first visit three years previously (C). US demonstrated presence of three well-defined, oval-shaped, homogenously hypoechoic masses within skin layer (white stars), with sizes of 9 × 4 mm, 8 × 5 mm and 4 × 2 mm, and mild posterior acoustic enhancement. As compared to previous US, current breast US (D) shows presence of masses that have apparently increased in size in skin and subcutaneous layer. Maximum diameter of masses had increased from 9 to 17 mm and from 8 to 9 mm. More importantly, three masses are surrounded by echogenic lines (white arrows) that represent dermal layer. This appearance suggests cutaneous lesion. E-H. Breast MRI demonstrates well-defined masses in left breast with low signal intensity on axial T1-weighted images (repetition time [TR]/echo time [TE]: 4.6/1.7) (E), intermediate- to low-signal intensity on T2-weighted turbo spin echo (TSE) images (TR/TE: 3800/90) (F), high signal intensity on turbo inversion recovery magnitude image (TIRM, TR/TE/inversion time [TI]: 5620/88/230) (G), and fat-suppressed gadolinium-enhanced T1-wighted image shows masses with homogeneous enhancement and linear structure that is biopsy needle track from skin to masses (H). I. Surgical specimen is 3.8 × 3.0 × 2.0 cm skin tissue specimen attached to breast tissue. There are two well-defined, yellow-white solid masses, 1.4 × 1.0 × 0.8 cm and 1.0 × 1.0 × 0.8 cm in size (arrows). J, K. Photomicrograph of specimen (Hematoxylin & Eosin staining) demonstrates eccrine spiradenoma composed of characteristic double population of outer small cells with darkly staining nuclei surrounding larger cells with pale cytoplasm and tightly packed cells arranged in jigsaw puzzle pattern without epidermal connections (original magnification, × 100 & × 400, respectively).
Reference
-
1. Kersting DW, Helwig EB. Eccrine spiradenoma. AMA Arch Derm. 1956. 73:199–227.2. Ribeiro-Silva A, Shaletich C, Careta RS, Kazava DK, Siqueira MC, Ponton F. Spiradenocarcinoma of the breast arising in a long-standing spiradenoma. Ann Diagn Pathol. 2004. 8:162–166.3. Leonard N, Smith D, McNamara P. Low-grade malignant eccrine spiradenoma with systemic metastases. Am J Dermatopathol. 2003. 25:253–255.4. Bosch MM, Boon ME. Fine-needle cytology of an eccrine spiradenoma of the breast: diagnosis made by a holistic approach. Diagn Cytopathol. 1992. 8:366–368.5. Han YD, Huan Y, Deng JL, Zhang YG, Zhang CH. MRI appearance of multiple eccrine spiradenoma. Br J Radiol. 2007. 80:E27–E29.6. Dijkhuizen T, van den Berg E, Nikkels PG, Hoekstra HJ, de Jong B. Cytogenetics of a case of eccrine spiradenoma. Hum Pathol. 1992. 23:1085–1087.7. Jin W, Kim GY, Lew BL, Yang DM, Kim HC, Ryu JK, et al. Sonographic findings of an eccrine spiradenoma: case report and literature review. J Ultrasound Med. 2008. 27:813–818.8. Hong SH, Chung HW, Choi JY, Koh YH, Choi JA, Kang HS. MRI findings of subcutaneous epidermal cysts: emphasis on the presence of rupture. AJR Am J Roentgenol. 2006. 186:961–966.9. Chen JT, Dahmash NS, Ravin CE, Heaston DK, Putman CE, Seigler HF, et al. Metastatic melanoma in the thorax: report of 130 patients. AJR Am J Roentgenol. 1981. 137:293–298.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Ruptured Epidermal Inclusion Cyst in the Breast Presenting as a Recurrent Abscess
- A Case of Giant Vascular Eccrine Spiradenoma
- A Case of Eccrine Spiradenoma on the Scrotum
- Treatment of Malignant Eccrine Spiradenoma
- Squamous Cell Carcinoma Arising from Epidermal Inclusion Cyst of Breast: Imaging Findings and Literature Review
