Fluoroscopy-Guided Percutaneous Gallstone Removal Using a 12-Fr Sheath in High-Risk Surgical Patients with Acute Cholecystitis
- Affiliations
-
- 1Department of Radiology, Keimyung University, College of Medicine, Daegu 700-712, Korea. yhkim68@dsmc.or.kr
- 2Institute for Medical Science, Keimyung University, Daegu 700-712, Korea.
- 3Department of Radiology, Andong General Hospital, Gyeongsangbuk-do 760-410, Korea.
- 4Department of Radiology, Gyeongsang National University, College of Medicine, Gyeongsangnam-do 660-702, Korea.
- KMID: 1088566
- DOI: http://doi.org/10.3348/kjr.2011.12.2.210
Abstract
OBJECTIVE
To evaluate the technical feasibility and clinical efficacy of percutaneous transhepatic cholecystolithotomy under fluoroscopic guidance in high-risk surgical patients with acute cholecystitis.
MATERIALS AND METHODS
Sixty-three consecutive patients of high surgical risk with acute calculous cholecystitis underwent percutaneous transhepatic gallstone removal under conscious sedation. The stones were extracted through the 12-Fr sheath using a Wittich nitinol stone basket under fluoroscopic guidance on three days after performing a percutaneous cholecystostomy. Large or hard stones were fragmented using either the snare guide wire technique or the metallic cannula technique.
RESULTS
Gallstones were successfully removed from 59 of the 63 patients (94%). Reasons for stone removal failure included the inability to grasp a large stone in two patients, and the loss of tract during the procedure in two patients with a contracted gallbladder. The mean hospitalization duration was 7.3 days for acute cholecystitis patients and 9.4 days for gallbladder empyema patients. Bile peritonitis requiring percutaneous drainage developed in two patients. No symptomatic recurrence occurred during follow-up (mean, 608.3 days).
CONCLUSION
Fluoroscopy-guided percutaneous gallstone removal using a 12-Fr sheath is technically feasible and clinically effective in high-risk surgical patients with acute cholecystitis.
MeSH Terms
-
Aged
Aged, 80 and over
Alloys
Cholecystitis, Acute/radiography/*surgery/ultrasonography
Cholecystostomy/*instrumentation
Conscious Sedation
Equipment Design
Feasibility Studies
Female
Fluoroscopy
Humans
Male
Middle Aged
Polyethylene
Polytetrafluoroethylene
Radiography, Interventional
Treatment Outcome
Ultrasonography, Interventional
Figure
-

Fig. 1 Picture of Wittich nitinol basket. Polyethylene portion of shaft (upper, arrow) was peeled off with blade (middle) in order to ease passage of stone basket and guide wire or metallic cannula (lower).

Fig. 2 83-year-old female with ruptured gallbladder empyema. A. Photograph of snare guide wire technique. B, C. Large stones were fragmented using snare guide wire technique. D. Cholecystogram obtained after stone extraction using Wittich nitinol stone basket showing complete stone clearance.
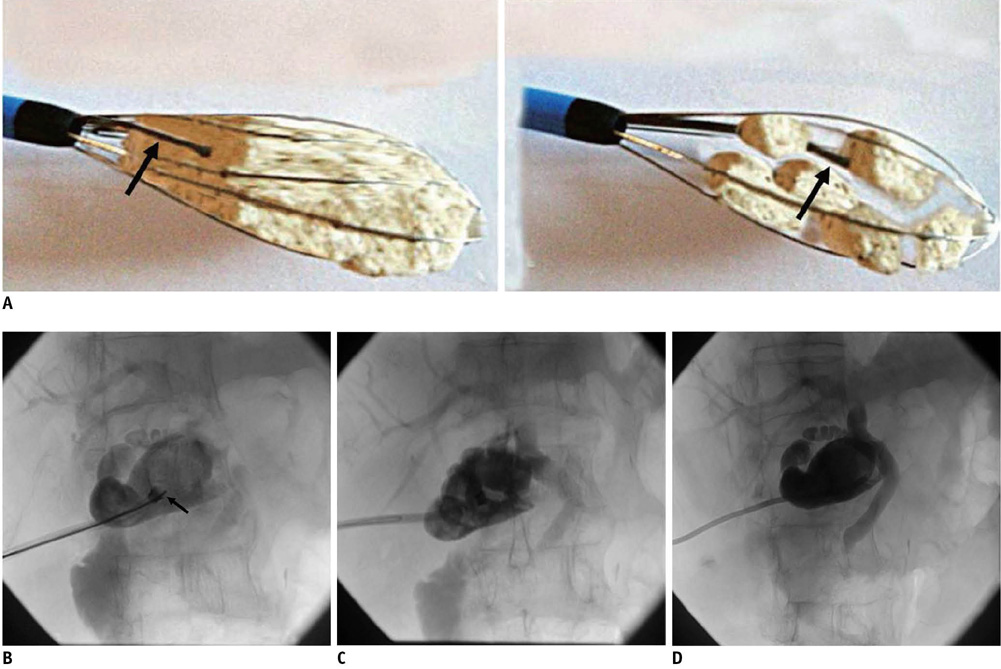
Fig. 3 81-year-old male with gallbladder empyema. A. Photograph of metallic cannula (arrow) technique. B. Hard stone being fragmented using metallic cannula (arrow) technique. C. Fragmented stones were extracted through 12-Fr sheath. D. Cholecystogram showing complete stone clearance and patent cystic duct.

Fig. 4 90-year-old male with acute cholecystitis. A. Cholecystogram showing multiple GB stones. B. Stones were successfully removed, but small stone remained in common bile duct (arrow). C. 12-Fr sheath was placed in common bile duct through cystic duct, and small common bile duct stone was extracted using Wittich stone basket.
Cited by 1 articles
-
Management of Acute Cholecystitis
Seung-Ok Lee, Sung Kyun Yim
Korean J Gastroenterol. 2018;71(5):264-268. doi: 10.4166/kjg.2018.71.5.264.
Reference
-
1. McDermott VG, Arger P, Cope C. Gallstone recurrence and gallbladder function following percutaneous cholecystolithotomy. J Vasc Interv Radiol. 1994. 5:473–478.2. Wong SK, Yu SC, Lam YH, Chung SS. Percutaneous cholecystostomy and endoscopic cholecystolithotripsy in the management of acute cholecystitis. Surg Endosc. 1999. 13:48–52.3. Picus D, Hicks ME, Darcy MD, Vesely TM, Kleinhoffer MA, Aliperti G, et al. Percutaneous cholecystolithotomy: analysis of results and complications in 58 consecutive patients. Radiology. 1992. 183:779–784.4. Lammert F, Miquel JF. Gallstone disease: from genes to evidence-based therapy. J Hepatol. 2008. 48:S124–S135.5. Melin MM, Sarr MG, Bender CE, van Heerden JA. Percutaneous cholecystostomy: a valuable technique in high-risk patients with presumed acute cholecystitis. Br J Surg. 1995. 82:1274–1277.6. Cheslyn-Curtis S, Russell RC. New trends in gallstone management. Br J Surg. 1991. 78:143–149.7. Cope C, Burke DR, Meranze SG. Percutaneous extraction of gallstones in 20 patients. Radiology. 1990. 176:19–24.8. Picus D, Marx MV, Hicks ME, Lang EV, Edmundowicz SA. Percutaneous cholecystolithotomy: preliminary experience and technical considerations. Radiology. 1989. 173:487–491.9. Kim HJ, Lee SK, Kim MH, Yoo KS, Lim BC, Seo DW, et al. Safety and usefulness of percutaneous transhepatic cholecystoscopy examination in high-risk surgical patients with acute cholecystitis. Gastrointest Endosc. 2000. 52:645–649.10. Gillams A, Curtis SC, Donald J, Russell C, Lees W. Technical considerations in 113 percutaneous cholecystolithotomies. Radiology. 1992. 183:163–166.11. Ohashi S. Percutaneous transhepatic cholecystoscopic lithotomy in the management of acute cholecystitis caused by gallbladder stones. Diagn Ther Endosc. 1998. 5:19–29.12. Bonnel DH, Liguory CE, Cornud FE, Lefebvre JF. Common bile duct and intrahepatic stones: results of transhepatic electrohydraulic lithotripsy in 50 patients. Radiology. 1991. 180:345–348.13. Park YS, Kim JH, Choi YW, Lee TH, Hwang CM, Cho YJ, et al. Percutaneous treatment of extrahepatic bile duct stones assisted by balloon sphincteroplasty and occlusion balloon. Korean J Radiol. 2005. 6:235–240.14. Gibney RG, Chow K, So CB, Rowley VA, Cooperberg PL, Burhenne HJ. Gallstone recurrence after cholecystolithotomy. AJR Am J Roentgenol. 1989. 153:287–289.15. Zou YP, Du JD, Li WM, Xiao YQ, Xu HB, Zheng F, et al. Gallstone recurrence after successful percutaneous cholecystolithotomy: a 10-year follow-up of 439 cases. Hepatobiliary Pancreat Dis Int. 2007. 6:199–203.16. Donald JJ, Cheslyn-Curtis S, Gillams AR, Russell RC, Lees WR. Percutaneous cholecystolithotomy: is gall stone recurrence inevitable? Gut. 1994. 35:692–695.17. So CB, Gibney RG, Scudamore CH. Carcinoma of the gallbladder: a risk associated with gallbladder-preserving treatments for cholelithiasis. Radiology. 1990. 174:127–130.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ectopic retained gallstone causing an abdominal wall abscess
- Endoscopic Gallbladder Drainage Conversion versus Conservative Treatment Following Percutaneous Gallbladder Drainage in High-Risk Surgical Patients
- Endoscopic Transpapillary Gallstone Removal with Recurrent Acute Cholecystitis
- Contracted Chronic Cholecystitis with Gallstone
- Management of Acute Cholecystitis
