Korean J Gastroenterol.
2011 Dec;58(6):318-322. 10.4166/kjg.2011.58.6.318.
The Safety of Early Enteral Feeding after Emergency Gastrointestinal Surgery
- Affiliations
-
- 1Department of Surgery, Yonsei University College of Medicine, Seoul, Korea. jakii@yuhs.ac
- 2Severance Hospital Nutrition Support Team, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1043330
- DOI: http://doi.org/10.4166/kjg.2011.58.6.318
Abstract
- BACKGROUND/AIMS
Postoperative early feeding has many advantages, and current guidelines recommend the early diet or enteral feeding after gastrointestinal surgery. However, there are controversies in emergency situation. The aim of this study was to assess the safety of early enteral feeding in patients underwent emergency gastrointestinal (GI) surgery.
METHODS
We reviewed the patients underwent emergency GI surgery by single surgeon from March 2008 to December 2010, retrospectively. The early feeding was defined when feeding was started within 72 hours after operation.
RESULTS
Fifty-three patients were enrolled. Men were 31, with mean 60.6 (+/-18.5) years old age. Thirty-three patients were treated in the intensive-care unit after operation. The most common cause of operation was bowel perforation, and followed by intestinal obstruction. Segmental resection with primary anastomosis of small bowel is the most common operation. Thirty-two of them started the diet within 48 hours postoperatively. Twenty-nine patients had post-operative complications. Wound complications were the most common, and followed by the abdominal pain, and ileus. Wound complications were developed in 18 patients, and the post-feeding abdominal pain was in 7 patients. Anastomotic leakage and intraabdominal abscess were developed in 2 patients, and 1 patient required reoperation to treat the anastomotic disruption. One patient developed pneumonia and sepsis, and resolved under conservative treatment. There was no mortality in these patients.
CONCLUSIONS
Early enteral feeding may be safe in cases of emergency GI surgery. However, it may require further studies to confirm the safety and feasibility of the early feeding in emergency situations.
Keyword
MeSH Terms
Figure
-
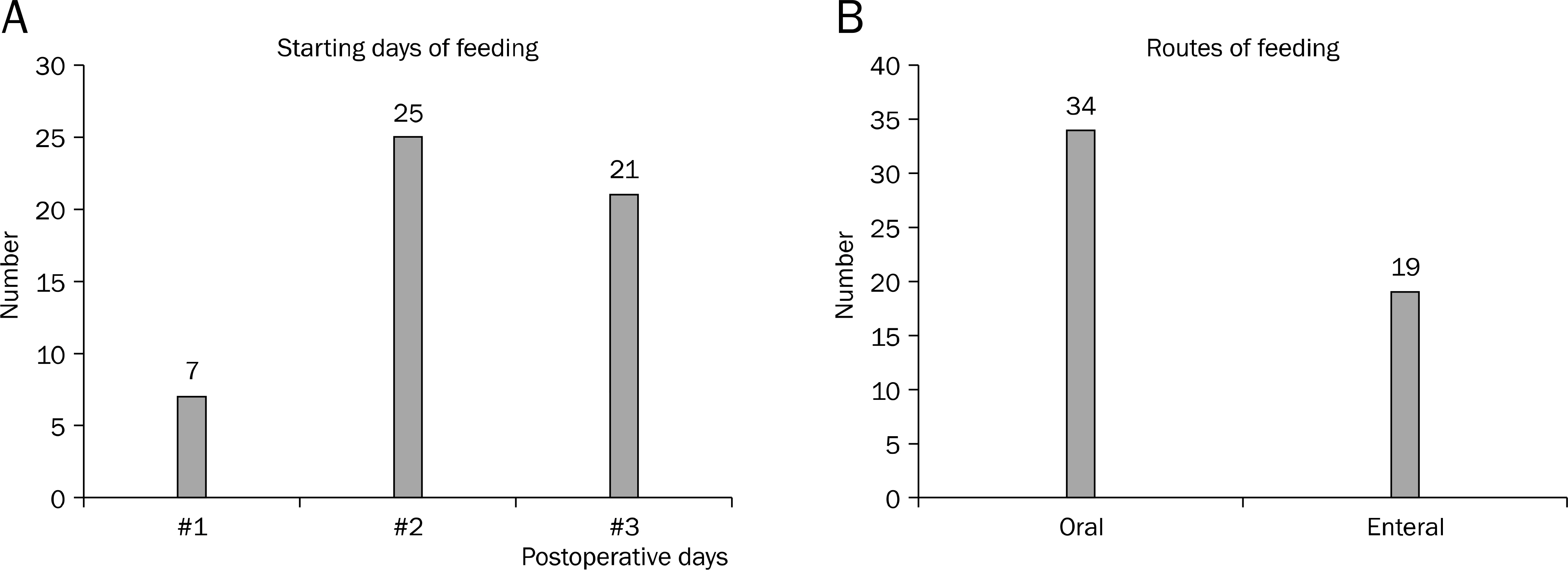
Fig. 1. Starting days (A) and routes of feeding (B).
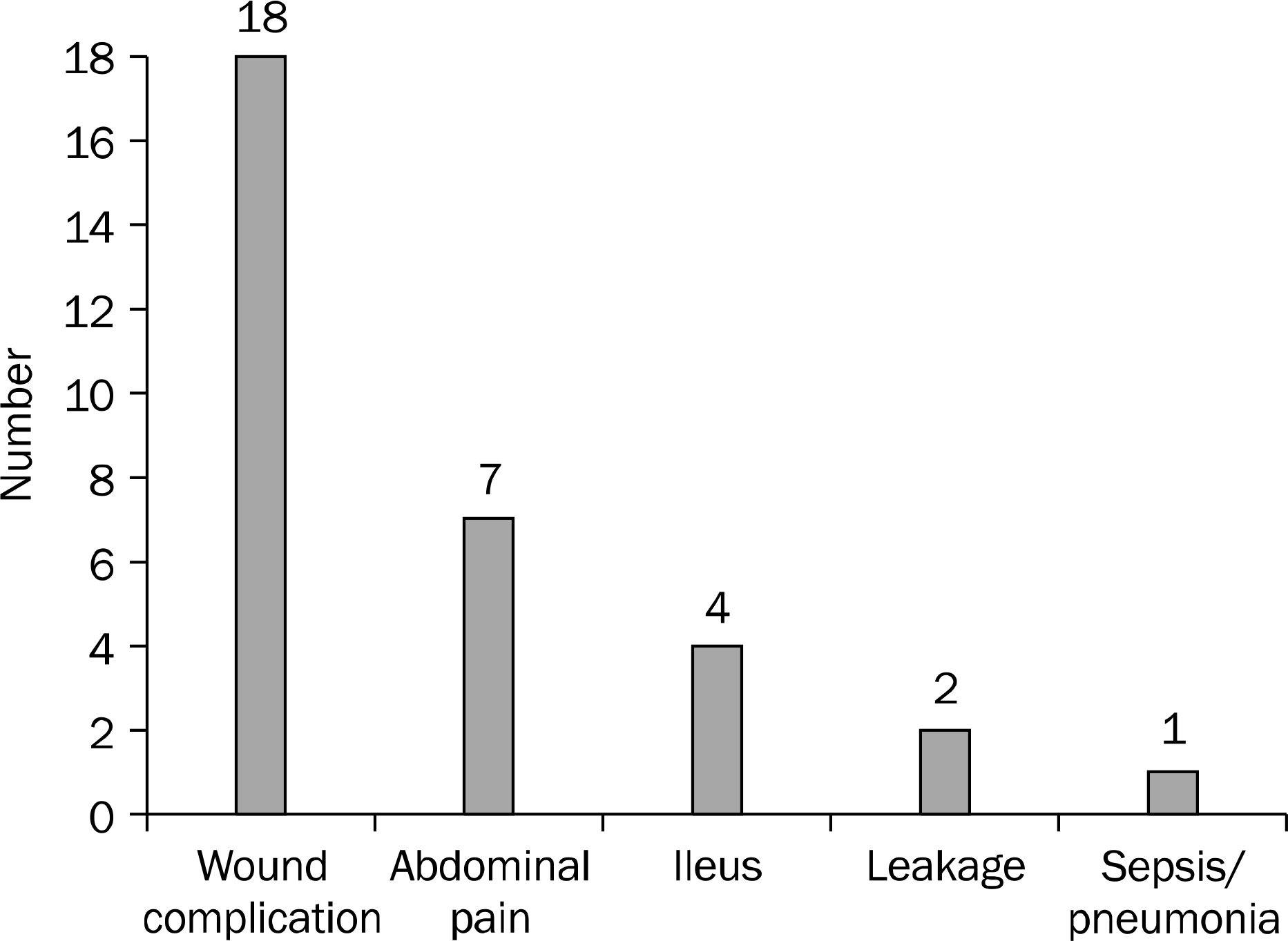
Fig. 2. Complications of early feeding after emergency gastrointestinal surgery.
Cited by 1 articles
-
Early Feeding Is Feasible after Emergency Gastrointestinal Surgery
Hyung Soon Lee, Hongjin Shim, Ji Young Jang, Hosun Lee, Jae Gil Lee
Yonsei Med J. 2014;55(2):395-400. doi: 10.3349/ymj.2014.55.2.395.
Reference
-
References
1. Dempsey DT, Mullen JL, Buzby GP. The link between nutritional status and clinical outcome: can nutritional intervention modify it? Am J Clin Nutr. 1988; 47(2 Suppl):352–356.
Article2. Giner M, Laviano A, Meguid MM, Gleason JR. In 1995 a correlation between malnutrition and poor outcome in critically ill patients still exists. Nutrition. 1996; 12:23–29.
Article3. Pennington CR, Powell-Tuck J, Shaffer J. Review article: artifi-cial nutritional support for improved patient care. Aliment Pharmacol Ther. 1995; 9:471–481.4. Pupelis G, Selga G, Austrums E, Kaminski A. Jejunal feeding, even when instituted late, improves outcomes in patients with severe pancreatitis and peritonitis. Nutrition. 2001; 17:91–94.
Article5. Lassen K, Soop M, Nygren J, et al. Enhanced Recovery After Surgery (ERAS) Group. Consensus review of optimal perioperative care in colorectal surgery: Enhanced Recovery After Surgery (ERAS) Group recommendations. Arch Surg. 2009; 144:961–969.6. Braga M, Ljungqvist O, Soeters P, Fearon K, Weimann A, Bozzetti F. ESPEN. ESPEN Guidelines on Parenteral Nutrition: surgery. Clin Nutr. 2009; 28:378–386.
Article7. Melis M, Fichera A, Ferguson MK. Bowel necrosis associated with early jejunal tube feeding: A complication of postoperative enteral nutrition. Arch Surg. 2006; 141:701–704.8. Zetti G, Tagliabue F, Barabino M, Fontana S, Ceppi M, Samori G. Small bowel necrosis associated with postoperative enteral feeding. Chir Ital. 2002; 54:555–558.9. Weimann A, Braga M, Harsanyi L, et al. ESPEN Guidelines on Enteral Nutrition: Surgery including organ transplantation. Clin Nutr. 2006; 25:224–244.
Article10. Wilmore DW, Long JM, Mason AD Jr, Skreen RW, Pruitt BA Jr. Catecholamines: mediator of the hypermetabolic response to thermal injury. Ann Surg. 1974; 180:653–669.11. Singh G, Ram RP, Khanna SK. Early postoperative enteral feeding in patients with nontraumatic intestinal perforation and peritonitis. J Am Coll Surg. 1998; 187:142–146.
Article12. Lewis SJ, Egger M, Sylvester PA, Thomas S. Early enteral feeding versus "nil by mouth" after gastrointestinal surgery: systematic review and metaanalysis of controlled trials. BMJ. 2001; 323:773–776.
Article13. Moore FA, Feliciano DV, Andrassy RJ, et al. Early enteral feeding, compared with parenteral, reduces postoperative septic complications. The results of a metaanalysis. Ann Surg. 1992; 216:172–183.
Article14. Marik PE, Zaloga GP. Early enteral nutrition in acutely ill patients: a systematic review. Crit Care Med. 2001; 29:2264–2270.
Article15. Shrikhande SV, Shetty GS, Singh K, Ingle S. Is early feeding after major gastrointestinal surgery a fashion or an advance? Evidence-based review of literature. J Cancer Res Ther. 2009; 5:232–239.
Article16. Kaur N, Gupta MK, Minocha VR. Early enteral feeding by na-soenteric tubes in patients with perforation peritonitis. World J Surg. 2005; 29:1023–1027.
Article
