A Case of Perforated Xanthogranulomatous Cholecystitis Presenting as Biloma
- Affiliations
-
- 1Department of Internal Medicine, Gyeongsang National University School of Medicine, Jinju, Korea. kimthy@medimail.co.kr
- 2Department of Pathology and Institute of Health Science, Gyeongsang National University School of Medicine, Jinju, Korea.
- KMID: 1018404
- DOI: http://doi.org/10.4166/kjg.2011.58.3.153
Abstract
- Xanthogranulomatous cholecystitis is an unusual inflammatory disease of the gallbladder characterized by severe proliferative fibrosis and the accumulation of lipid-laden macrophages in areas of destructive inflammation. Its macroscopic appearance may occasionally be confused with gallbladder carcinoma. We present a case of perforated xanthogranulomatous cholecystitis presenting as biloma. An 80-year-old woman was referred to our hospital with a 1-week history of abdominal pain and febrile sensation. Abdominal CT showed a biloma in the subhepatic area. The follow-up CT showed that the biloma increased in size. Therefore, ultrasonography-guided aspiration was performed. The aspirated fluid/serum bilirubin ratio was greater than 5, which was strongly suggestive of bile leakage complicated by perforated cholecystitis. She underwent a laparoscopic cholecystectomy with cyst aspiration and adhesiolysis. A histological diagnosis of perforated xanthogranulomatous cholecystitis was made.
MeSH Terms
Figure
-
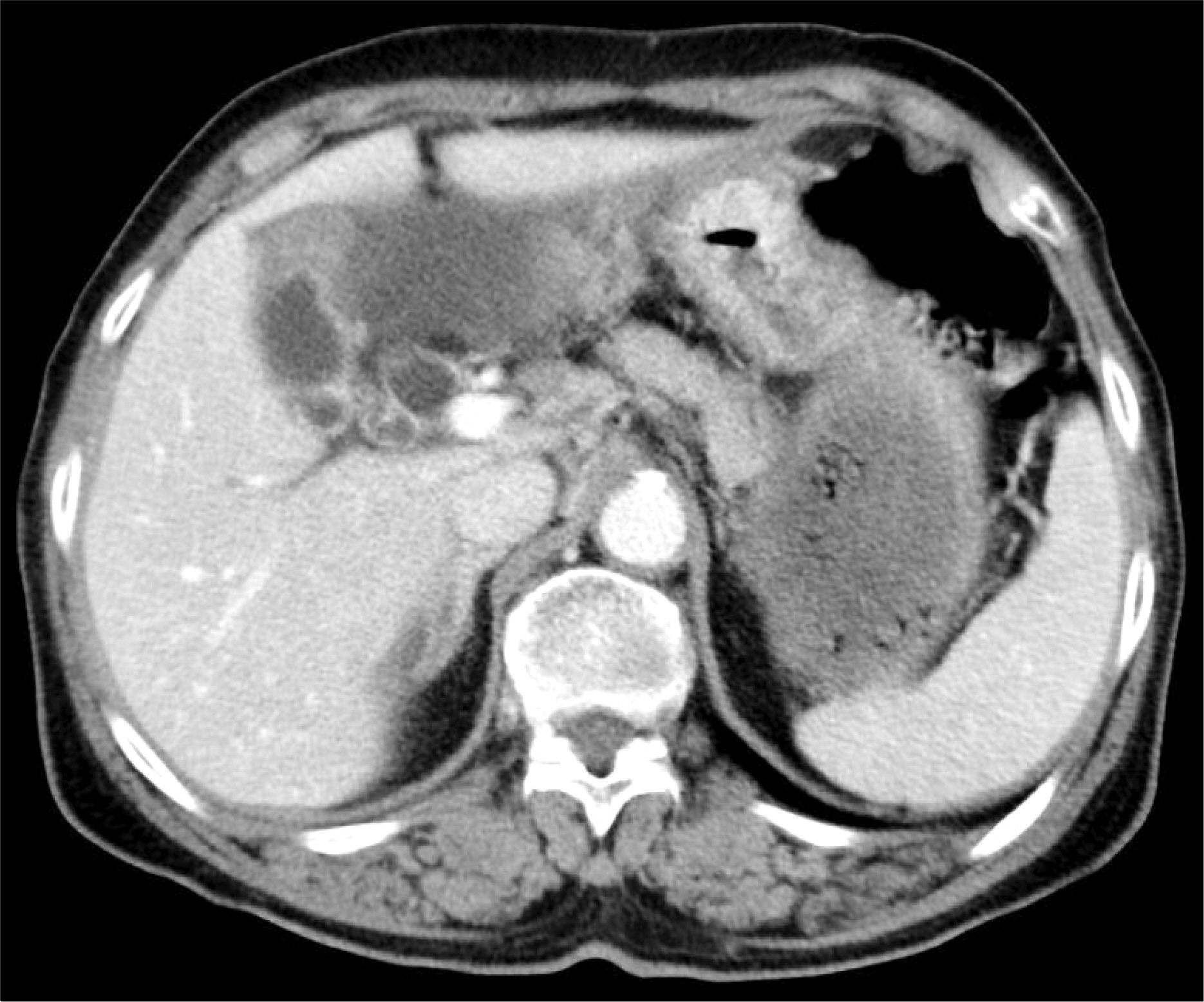
Fig. 1. CT scan of abdomen. It showed a focal gallbladder wall thickening and fluid collection in the subhepatic space. There was no definitive connection between the fluid collection and the gallbladder.

Fig. 2. Follow-up CT scan of abdomen. It showed that the cystic mass increased in size (11×5 cm) with wall enhancement in the subhepatic space.
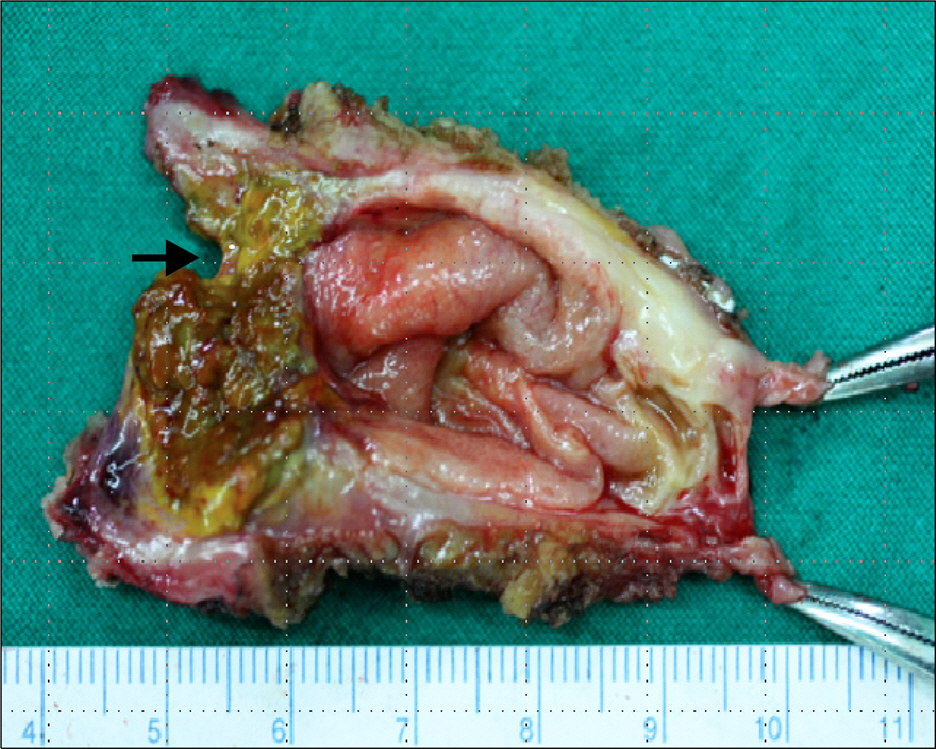
Fig. 3. Gross findings of the specimen. The gallbladder was characterized by a thickened wall with poorly circumscribed yellowish granular necrotic areas and perforation (arrow).

Fig. 4. Microscopic findings of the specimen. (A) The ulcerated mucosa of the gallbladder was stained with bile pigments (H&E stain, ×40). (B) The subepithelial connective tissue of the gallbladder showed a massive aggregation of foamy macrophages. There were also infiltration of lymphocytes, plasma cells and occasional multinucleated giant cells. Many macrophages contained both ceroid pigments and cholesterol (H&E stain, ×400).
Reference
-
References
1. Hanada K, Nakata H, Nakayama T, et al. Radiologic findings in xanthogranulomatous cholecystitis. AJR Am J Roentgenol. 1987; 148:727–730.
Article2. Parra JA, Acinas O, Bueno J, Güezmes A, Fernández MA, Fariñas MC. Xanthogranulomatous cholecystitis: clinical, sonographic, and CT findings in 26 patients. AJR Am J Roentgenol. 2000; 174:979–983.3. Roberts KM, Parsons MA. Xanthogranulomatous cholecystitis: clinicopathological study of 13 cases. J Clin Pathol. 1987; 40:412–417.
Article4. Seo SH, Park JI, Kim JS, Kim KH, Choi CS, Choi YK. Xanthogranulomatous cholecystitis: a retrospective analysis of 36 cases. J Korean Surg Soc. 2009; 76:371–377.
Article5. Kim HY, Cho YH, Park JH. Xanthogranulomatous cholecystitis not associated with gallstone in a 9-year-old girl. J Korean Surg Soc. 2009; 77:72–74.
Article6. Joo YE, Lee JJ, Chung IJ, et al. A case of xanthogranulomatous cholecystitis. Korean J Intern Med. 1999; 14:90–93.
Article7. Kim DS, Choi DY, Kim YS, et al. A case of xanthogranulomatous cholecystitis associated with Mirizzi syndrome. Korean J Gastroenterol. 1999; 34:136–141.8. Kim PN, Ha HK, Kim YH, Lee MG, Kim MH, Auh YH. US findings of xanthogranulomatous cholecystitis. Clin Radiol. 1998; 53:290–292.
Article9. Kim KH, Ahn CH, Kim JS, et al. Xanthogranulomatous cholecystitis mimicking gallbladder cancer. J Korean Surg Soc. 2002; 63:441–444.10. Lee HS, Joo KR, Kim DH, et al. A case of simultaneous xanthogranulomatous cholecystitis and carcinoma of the gallbladder. Korean J Intern Med. 2003; 18:53–56.
Article11. Houston JP, Sampson MA, Collins MC. Ultrasound diagnosis of gallbladder perforation in a case of xanthogranulomatous cholecystitis. Br J Radiol. 1989; 62:273–274.
Article12. Hsu C, Hurwitz JL, Schuss A, Katz DS. Radiology-pathology conference: xanthogranulomatous cholecystitis. Clin Imaging. 2003; 27:421–425.13. Khan SA, Gulfam , Anwer AW, Arshad Z, Hameed K, Shoaib M. Gallbladder perforation: a rare complication of acute cholecystitis. J Pak Med Assoc. 2010; 60:228–229.14. Darwin P, Goldberg E, Uradomo L. Jackson Pratt drain fluid-to-serum bilirubin concentration ratio for the diagnosis of bile leaks. Gastrointest Endosc. 2010; 71:99–104.
Article15. Runyon BA. Ascitic fluid bilirubin concentration as a key to choleperitoneum. J Clin Gastroenterol. 1987; 9:543–545.
Article16. Welsch T, von Frankenberg M, Schmidt J, Büchler MW. Diagnosis and definition of anastomotic leakage from the surgeon's perspective. Chirurg. 2011; 82:48–55.17. Antolovic D, Koch M, Galindo L, et al. Hepaticojejunostomy–an-alysis of risk factors for postoperative bile leaks and surgical complications. J Gastrointest Surg. 2007; 11:555–561.
Article
