Repositioning of a Free Cap after Laser-assisted in situ Keratomileusis
- Affiliations
-
- 1Saevit Eye Hospital, Goyang, Korea. zenith716@gmail.com
- KMID: 2411459
- DOI: http://doi.org/10.3341/jkos.2018.59.5.484
Abstract
- PURPOSE
To report a case of irregular astigmatism caused by a free flap during laser-assisted in situ keratomileusis (LASIK) surgery that was treated with a flap rotation based on postoperative topography.
CASE SUMMARY
A 21-year-old female underwent LASIK, which was complicated by a free cap on her right eye. Because the gentian violet markings were no longer present, the exact orientation of the cap was unknown. At 3 months after surgery, the astigmatism of the right eye was −3.00 diopters (D) with an uncorrected visual acuity (UCVA) of 0.4, and the astigmatism of the left eye was −0.75 D with an UCVA of 1.0. The corneal topography was analyzed in order to return to the existing position. Free cap repositioning was performed and irregular astigmatism was corrected to improve the UCVA to 1.0.
CONCLUSIONS
If the preoperative markings cannot be identified on a free flap during LASIK, secondary postoperative corneal topographic analysis can be performed to restore the corneal free flap to its original position to minimize astigmatism with good visual outcomes.
MeSH Terms
Figure
-

Figure 1. Topography measured before laser-assisted in situ keratomileusis (LASIK). (A) Preoperative Pentacam®, front sagittal curvature maps of both eyes show with the rule astigmatism. (B) Preoperative Orbscan. Anterior elevation maps of both eyes show with the rule astigmatism. OD = oculus dexter; OS = oculus sinister; Sim K = simulated keratometry; Astig = astigmatism; T = temporal; N = nasal.

Figure 2. Topography measured after laser-assisted in situ keratomileusis (LASIK). (A) Pentacam® measured 3 months after LASIK of both eyes and before flap reposition of right eye, frontal corneal astigmatism is −3.2 D on right eye. (B) Orbscan measured 3 months after LASIK of both eyes and before flap reposition of right eye, front sagittal curvature maps of both eyes show with the rule astigmatism. OD = oculus dexter; OS = oculus sinister; Sim K = simulated keratometry; Astig = astigmatism; T = temporal; N = nasal.
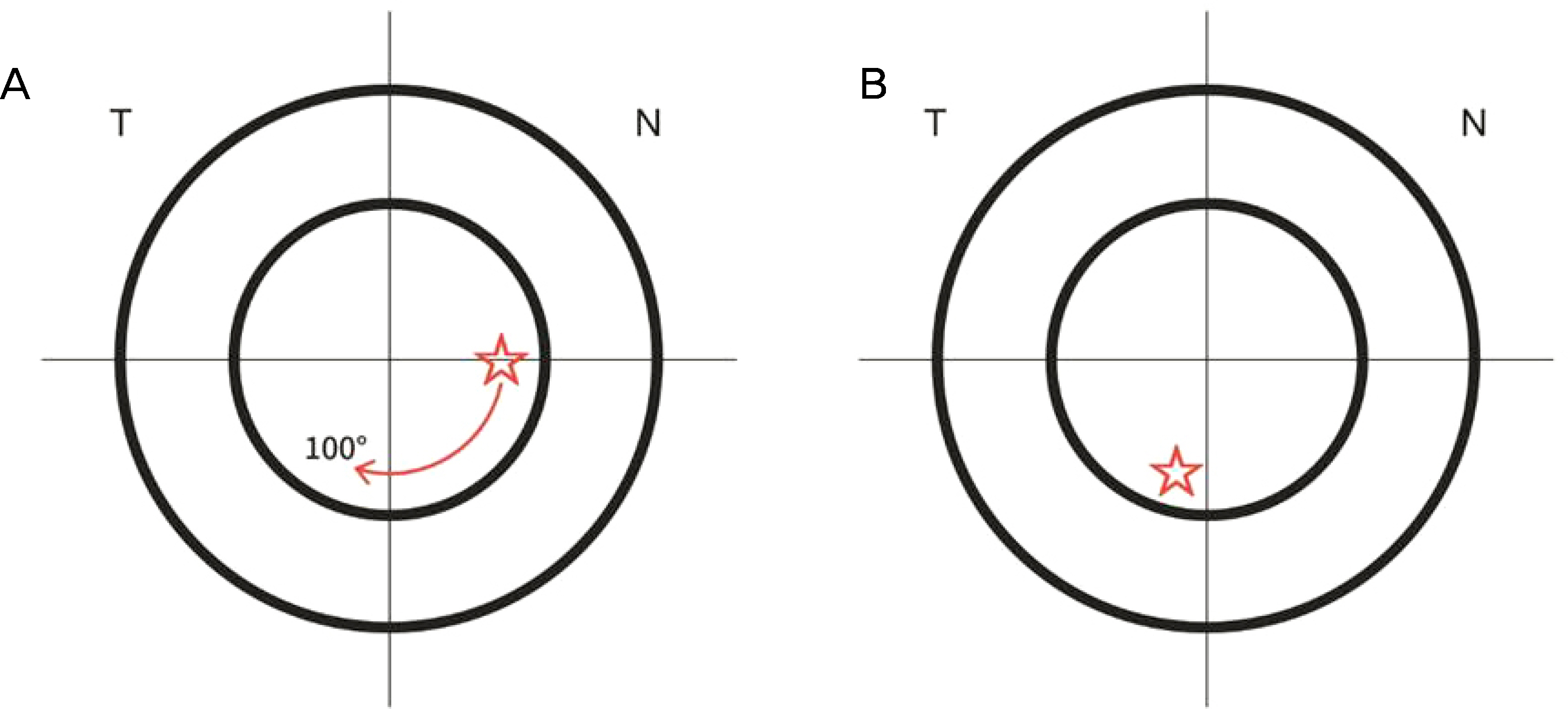
Figure 3. The schematic figure of reposition procedures. (A) Detachment of prepositioned free cap and dialing 100 degrees clockwise. (B) Reposition of free cap. In both figures, ‘T’ represents the temporal side of eye and ‘N’ represents the nasal side of eye. The red star on (A) and (B) represents marking for same location of flap. The red arrow on (A) represents degrees of flap rotation.
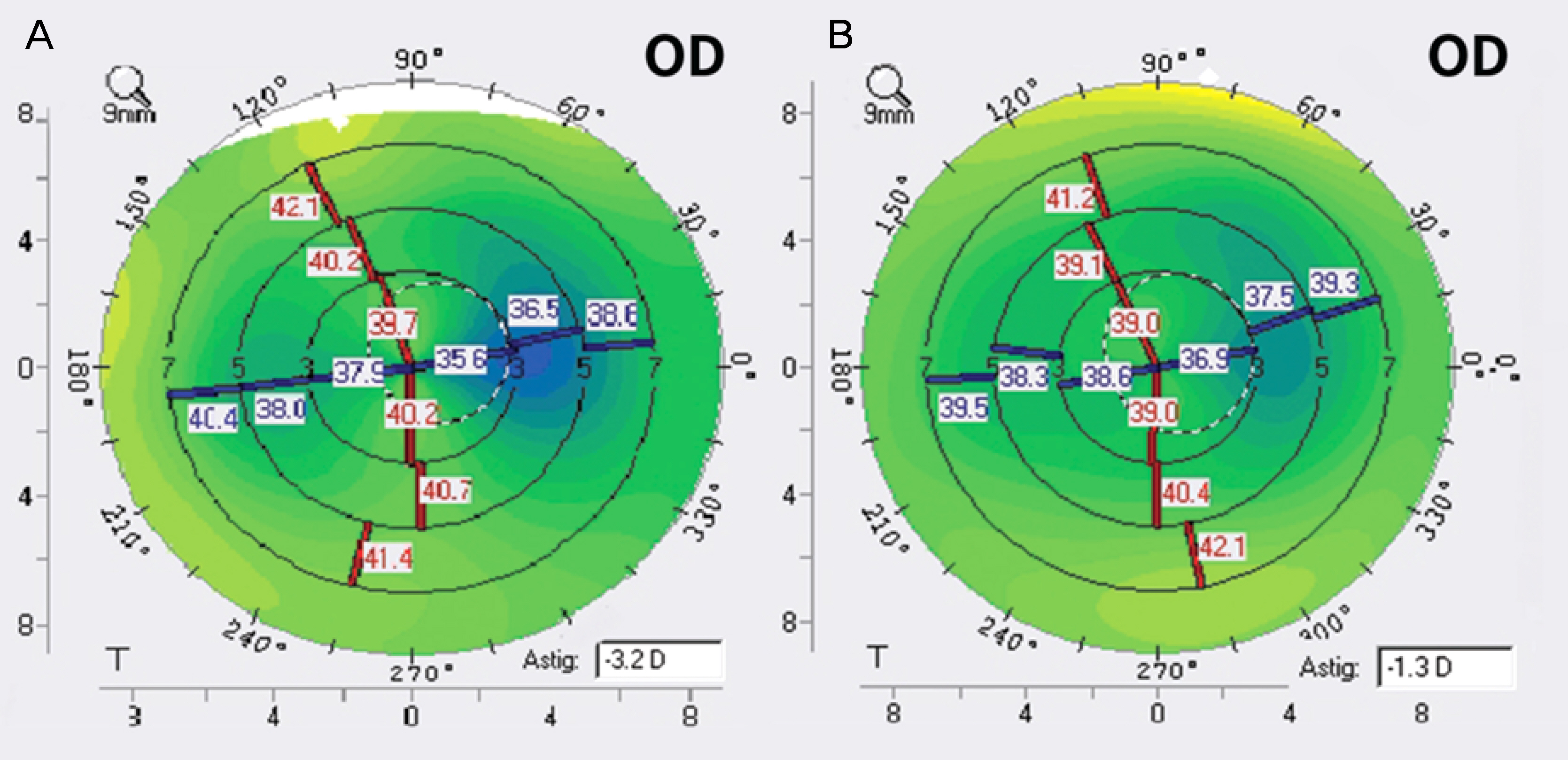
Figure 4. Topography measured before and after flap reposition. (A) Pentacam® measured after laser-assisted in situ keratomileusis (LASIK) (before flap reposition) of right eye, frontal corneal astigmatism is −3.2 D on right eye. (B) Pentacam® measured 1 month after flap reposition of right eye, frontal corneal astigmatism is −1.3 D on right eye. OD = oculus dexter; Astig = astigmatism; T = temporal.
Reference
-
References
1. Romero-Diaz-de-Leon L, Serna-Ojeda JC, Navas A, et al. Intraoperative flap complications in LASIK surgery performed by ophthalmology residents. J Ophthalmic Vis Res. 2016; 11:263–7.
Article2. Jacobs JM, Taravella MJ. Incidence of intraoperative flap abdominals in laser in situ keratomileusis. J Cataract Refract Surg. 2002; 28:23–8.3. Karabela Y, Muftuoglu O, Gulkilik IG, et al. Intraoperative and early postoperative flap-related complications of laser in situ abdominal using two types of Moria microkeratomes. Int Ophthalmol. 2014; 34:1107–14.4. Ahn JY, Kwon JW, Lee SM, et al. Comparison of the flap abdominal rate between microkeratomes for LASIK. J Korean Ophthalmol Soc. 2008; 49:1425–30.5. Cheng AC, Wong VW, Rao SK, Lam DS. Repositioning of free cap four days after LASIK. J Refract Surg. 2007; 23:625–7.
Article6. Nakano K, Nakano E, Oliveira M, et al. Intraoperative abdominal complications in 47,094 laser in situ keratomileusis surgeries. J Refract Surg. 2004; 20(5 Suppl):S723–6.
Article7. Carrillo C, Chayet AS, Dougherty PJ, et al. Incidence of complications during flap creation in LASIK using the Nidek MK-2000 abdominal in 26,600 cases. J Refract Surg. 2005; 21(5 Suppl):S655–7.
Article8. Hovanesian JA, Maloney RK. Treating astigmatism after a free abdominal in situ keratomileusis cap by rotating the cap. J Cataract Refract Surg. 2005; 31:1870–6.9. Utz VM, Krueger RR. Management of irregular astigmatism following rotationally disoriented free cap after LASIK. J Refract Surg. 2008; 24:383–91.
Article10. Lee JB, Seong GJ, Lee JH, et al. Comparison of laser epithelial abdominal and photorefractive keratectomy for low to moderate myopia. J Cataract Refract Surg. 2001; 27:565–70.11. McLeod SD, Holsclaw D, Lee S. Refractive, topographic, and abdominal effects of flap amputation following laser in situ keratomileusis. Arch Ophthalmol. 2002; 120:1213–7.12. Hashmani S, Hashmani N, Rajani H, et al. Comparison of visual acuity, refractive outcomes, and satisfaction between LASIK abdominal with a microkeratome and a femto laser. Clin Ophthalmol. 2017; 11:1009–14.13. Pietilä J, Huhtala A, Jääskeläinen M, et al. LASIK flap creation with the Ziemer femtosecond laser in 787 consecutive eyes. J Refract Surg. 2010; 26:7–16.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ocular deviation after unilateral laser in situ keratomileusis
- 6 Cases of Vision Threatening Keratitis following Laser in Situ Keratomileusis
- Corneal Keloid Case after Laser-assisted in-situ Keratomileusis Surgery in Korea
- Coniparision of Clinical Results Between Keratomileusis In Situ and Laser Assisted In Situ Keratomileusis for High Myopia from -15 Diopter to -23 Diopter
- Change of Values of Intraocular Pressures Measurements after Laser In Situ Keratomileusis
