Feasibility and Utility of Transradial Cerebral Angiograpy: Experience during the Learning Period
- Affiliations
-
- 1Department of Diagnostic Radiology, Konyang University Hospital, Daejeon, Korea. radol@unitel.co.kr
- 2Department of Neurosurgery, Konyang University Hospital, Daejeon, Korea.
- KMID: 753910
- DOI: http://doi.org/10.3348/kjr.2006.7.1.7
Abstract
OBJECTIVE
We wanted to present our experiences for performing transradial cerebral angiography during the learning period, and we also wanted to demonstrate this procedure's technical feasibility and utility in various clinical situations. MATERIALS AND METHODS: Thirty-two patients were enrolled in the study. All of them had unfavorable situations for performing transfemoral angiography, i.e., IV lines in the bilateral femoral vein, a phobia for groin puncture, decreased blood platelet counts, large hematoma or bruise, atherosclerosis in the bilateral femoral artery and the insistence of patients for choosing another procedure. After confirming the patency of the ulnar artery with a modified Allen's test and a pulse oximeter, the procedure was done using a 21-G micorpuncture set and 5-F Simon II catheters. After angiography, hemostasis was achieved with 1-2 minutes of manual compression and the subsequent application of a hospital-made wrist brace for two hours. The technical feasiblity and procedure-related immediate and delayed complications were evaluated. RESULTS: The procedure was successful in 30/32 patients (93.8%). Failure occurred in two patients; one patient had hypoplasia of the radial artery and one patient had vasospasm following multiple puncture trials for the radial artery. Transradial cerebral angiography was technically feasible without significant difficulties even though it was tried during the learning period. Pain in the forearm or arm developed in some patients during the procedures, but this was usually mild and transient. Procedure-related immediate complications included severe bruising in one patient and a small hematoma in one patient. Any clinically significant complication or delayed complication such as radial artery occlusion was not demonstrated in our series. CONCLUSION: Transradial cerebral angiography is a useful alternative for the patients who have unfavorable clinical situations or contraindications for performing transfemoral cerebral angiography. For the experienced neurointerventionalists, it seems that additional training for perfoming transradial cerebral angiography is not needed.
Keyword
MeSH Terms
Figure
-
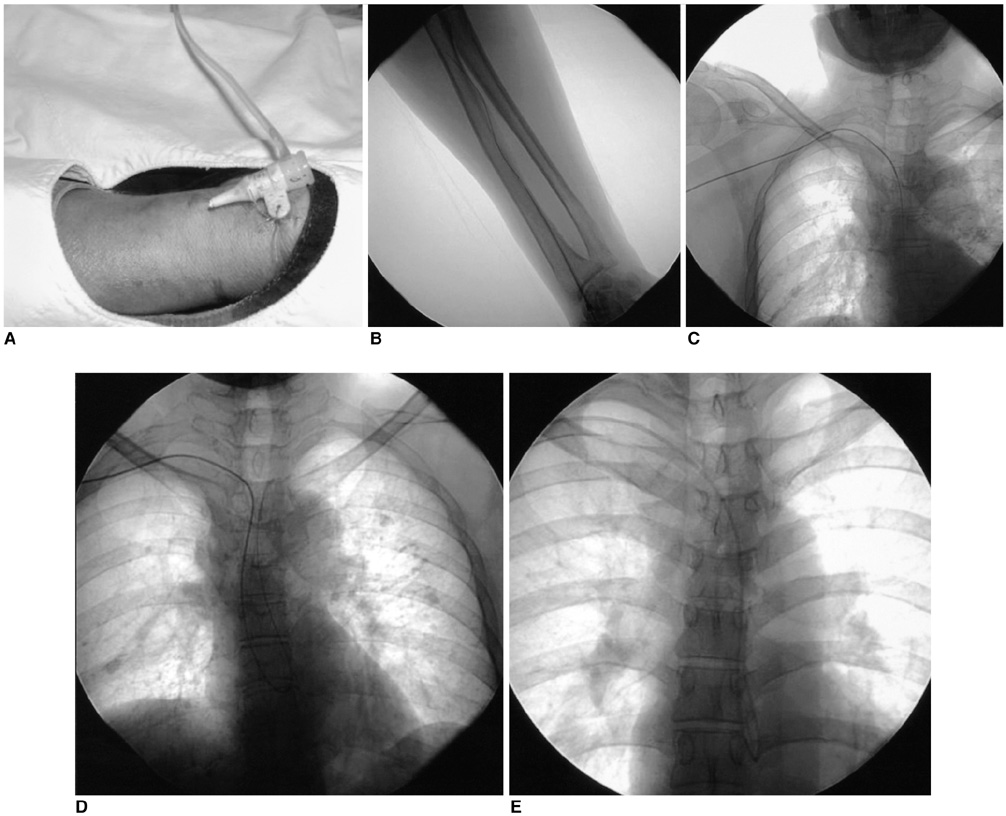
Fig. 1 Due to groin phobia, this 44-year-old male patient underwent transradial cerebral angiography. A. A 5-F introducer sheath was inserted into the radial artery. B. A 0.035-inch guide wire was passed though the radial and brachial arteries. C. A guide wire and a 5-F Simon II catheter were introduced into the ascending aorta. D. The guide wire was turned back at the aortic valve. E. A J-curve was made at the distal portion of the Simon II catheter.
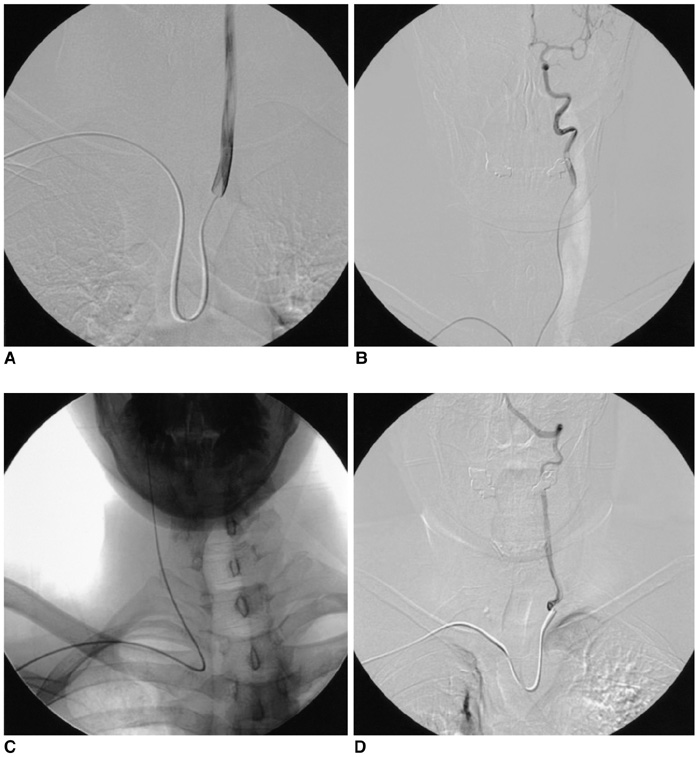
Fig. 2 When handling the catheter, the brain supplying arteries can be easily selected. A. Left common carotid artery, B. Left internal carotid artery, C. Right common and internal carotid artery, D. Left vertebral artery.
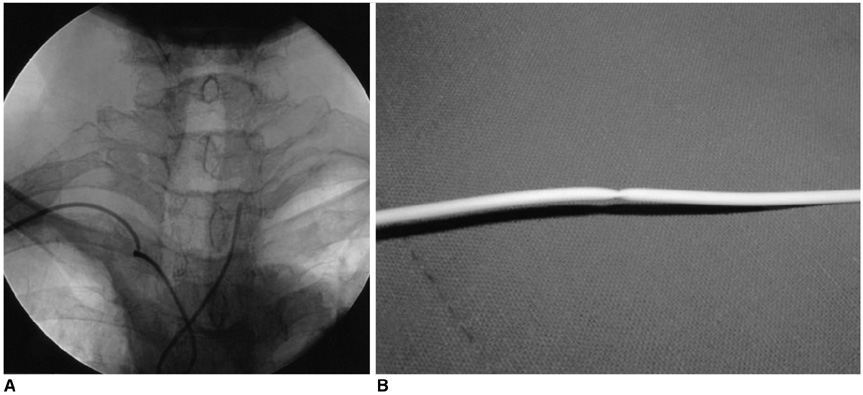
Fig. 3 A. During catheter handling to select the right common carotid artery, the catheter kinked because of excessive torque. The innominate artery was very tortuous in this patient. B. The catheter was withdrawn. Focal kinking is demonstrated in the catheter.
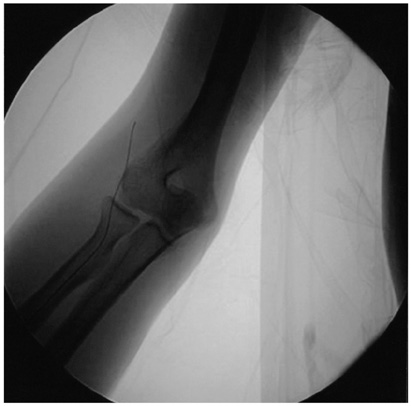
Fig. 4 During guide wire insertion through the radial artery, it entered the radial recurrent artery, causing sharp pain in the forearm.
Cited by 1 articles
-
Efficacy of Transradial Cerebral Angiography in the Elderly
Jung-Hyun Park, Dae-Yong Kim, Jin-Wook Kim, Yong-Seok Park, Won-Bae Seung
J Korean Neurosurg Soc. 2013;53(4):213-217. doi: 10.3340/jkns.2013.53.4.213.
Reference
-
1. Hildick-Smith DJR, Khan ZI, Shapiro LM, Petch MC. Occasional operator percutaneous brachial coronary angiography: first, do no arm. Catheter Cardiovasc Interv. 2002. 57:155–161.2. McIvor J, Rhymer JC. 245 transaxillary arteriograms in arteriopathic patients: success rate and complications. Clin Radiol. 1992. 45:390–394.3. Campeau L. Percutaneous radial artery approach for coronary angiography. Cathet Cardiovasc Diagn. 1989. 16:3–7.4. Ludman PF, Stephens NG, Harcombe A, Lowe MD, Shapiro LM, Schofield PM, et al. Radial versus femoral approach for diagnostic coronary angiography in stable angina pectoris. Am J Cardiol. 1997. 79:1239–1241.5. Hildick-Smith DJR, Lowe MD, Walsh JT, Ludman PF, Stephens NG, Schofield PM, et al. Coronary angiography from the radial artery: experience, complications and limitations. Int J Cardiol. 1998. 64:231–239.6. Kiemeneij F, Laarman GJ. Transradial artery Palmaz-Schatz coronary stent implantation: results of a single-center feasibility study. Am Heart J. 1995. 130:14–21.7. Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der Wieken R. A randomized comparison of percutaneous transluminal coronary angioplasty by the radial, brachial and femoral approaches: the ACCESS study. J Am Coll Cardiol. 1997. 29:1269–1275.8. Laarman G, Muthusamy TS, Swart H, Westendorp I, Kiemeneij F, Slagboom T, et al. Direct coronary stent implantation: safety, feasibility, and predictors of success of the strategy of direct coronary stent implantation. Catheter Cardiovasc Interv. 2001. 52:443–448.9. Sharma GL, Loubeyre C, Morice MC. Safety and feasibility of the radial approach for primary angioplasty in acute myocardial infarction during pregnancy. J Invas Cardiol. 2002. 14:359–362.10. Mann T. The radial approach for coronary angiography and stenting. Heart. 1999. 82:411–412.11. Matsumoto Y. Transradial approach for selective cerebral angiography: technical note. Neurol Res. 2000. 22:605–608.12. Matsumoto Y, Hongo K, Toriyama T, Nagashima H, Kobayashi S. Transradial approach for diagnostic selective cerebral angiography: results of a consecutive series of 166 cases. AJNR Am J Neuroradiol. 2001. 22:704–708.13. Nohara AM, Kallmes DF. Transradial cerebral angiography: technique and outcomes. AJNR Am J Neuroradiol. 2003. 24:1247–1250.14. Fessler RD, Wakhloo AK, Lanzino G, Guterman LR, Hopkins LN. Transradial approach for vertebral artery stenting: technical case report. Neurosurgery. 2000. 46:1524–1527.15. Yoo BS, Lee SH, Kim JY, Lee HH, Ko JY, Lee BK, et al. A case of transradial carotid stenting in a patient with total occlusion of distal abdominal aorta. Catheter Cardiovasc Interv. 2002. 56:243–245.16. Lee DH, Ahn JH, Jeong SS, Eo KS, Park MS. Routine transradial access for conventional cerebral angiography: a single operator's experience of its feasibility and safety. Br J Radiol. 2004. 77:831–838.17. Hildick-Smith DJ, Walsh JT, Lowe MD, Shapiro LM, Petch MC. Transradial coronary angiography in patients with contraindications to the femoral approach: an analysis of 500 cases. Catheter Cardiovasc Interv. 2004. 61:60–66.18. Nagai S, Abe S, Sato T, Hozawa K, Yuki K, Hanashima K, et al. Ultrasonic assessment of vascular complications in coronary angiography and angioplasty after transradial approach. Am J Cardiol. 1999. 83:180–186.19. Louvard Y, Lefevre T, Allain A, Morice M. Coronary angiography through the radial or the femoral approach: the CARAFE study. Catheter Cardiovasc Interv. 2001. 52:181–187.20. Louvard Y, Krol M, Pezzano M, Sheers L, Piechaud JF, Marien C, et al. Feasibility of routine transradial coronary angiography: a single operator's experience. J Invasive Cardiol. 1999. 11:543–548.21. Kiemeneij F, Laarman GJ, Slagboom T, van der Wieken R. Outpatient coronary stent implantation. J Am Coll Cardiol. 1997. 29:323–327.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Is Transradial Cerebral Angiography Feasible and Safe? A Single Center's Experience
- Feasibility and Problems in Transradial Coronary Angiography and Intervention
- Efficacy of Transradial Cerebral Angiography in the Elderly
- Transradial Approach for Thoracolumbar Spinal Angiography and Tumor Embolization: Feasibility and Technical Considerations
- The Effect of Self-directed Learning Strategies on e-Learning Pre-learning of Nursing Students: Focusing on the Flow Experience
