Real-world effectiveness of a single conventional diseasemodifying anti-rheumatic drug (cDMARD) plus an anti-TNF agent versus multiple cDMARDs in rheumatoid arthritis: a prospective observational study
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea
- 2Division of Rheumatology, Department of Internal Medicine, Keimyung University Dongsan Hospital, Daegu, Korea
- 3Division of Rheumatology, Department of Internal Medicine, Inje University Busan Paik Hospital, Busan, Korea
- 4Department of Rheumatology, Hanyang University Hospital for Rheumatic Diseases, Seoul, Korea
- 5Division of Rheumatology, Department of Internal Medicine, Daegu Catholic University School of Medicine, Daegu, Korea
- 6Department of Internal Medicine and Institute of Health Science, Gyeongsang National University School of Medicine and Hospital, Jinju, Korea
- 7Department of Internal Medicine, Eulji University College of Medicine, Seoul, Korea
- 8Division of Rheumatology, Department of Internal Medicine, Hanyang University Guri Hospital, Guri, Korea
- 9Division of Rheumatology, Department of Internal Medicine, Konkuk University Medical Center, Seoul, Korea
- 10Medical Department, MSL, Eisai Korea Inc., Seoul, Korea
- KMID: 2554324
- DOI: http://doi.org/10.4078/jrd.2023.0045
Abstract
Objective
The objective of this prospective, observational multicenter study (NCT03264703) was to compare the effectiveness of single conventional disease-modifying anti-rheumatic drug (cDMARD) plus anti-tumor necrosis factor (TNF) therapy versus multiple cDMARD treatments in patients with moderate-to-severe rheumatoid arthritis (RA) following cDMARD failure in the real-world setting in South Korea.
Methods
At the treating physicians’ discretion, patients received single cDMARD plus anti-TNF therapy or multiple cDMARDs. Changes from baseline in disease activity score 28-joint count with erythrocyte sedimentation rate (DAS28-ESR), corticosteroid use, and Korean Health Assessment Questionnaire (KHAQ-20) scores were evaluated at 3, 6, and 12 months.
Results
Of 207 enrollees, the final analysis included 45 of 73 cDMARD plus anti-TNF and 91 of 134 multiple-cDMARD recipients. There were no significant between-group differences (BGDs) in ANCOVA-adjusted changes from baseline in DAS28-ESR at 3, 6 (primary endpoint), and 12 months (BGDs −0.18, −0.38, and −0.03, respectively). More cDMARD plus anti-TNF than multiple-cDMARD recipients achieved a >50% reduction from baseline in corticosteroid dosage at 12 months (35.7% vs 14.6%; p=0.007). Changes from baseline in KHAQ-20 scores at 3, 6, and 12 months were significantly better with cDMARD plus antiTNF therapy than with multiple cDMARDs (BGD −0.18, −0.19, and −0.19 points, respectively; all p≤0.024).
Conclusion
In the real-world setting, relative to multiple cDMARDs, single cDMARD plus anti-TNF therapy significantly improved quality-of-life scores and reduced corticosteroid use, with no significant BGD in disease activity, in RA patients in whom previous cDMARD therapy had failed.
Keyword
Figure
-
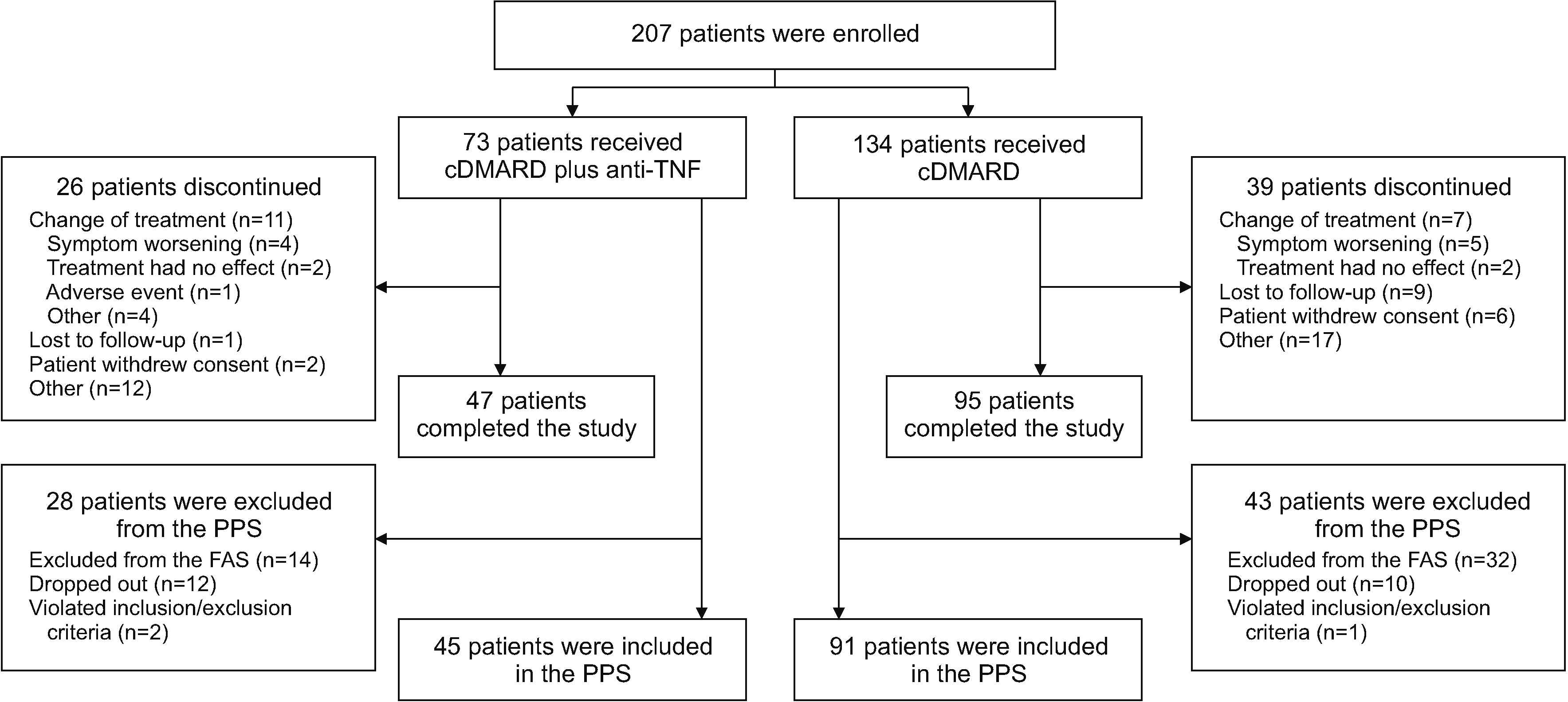
Figure 1 Patient disposition. Anti-TNF: anti-tumor necrosis factor agent, cDMARD: conventional disease-modifying anti-rheumatic drug, FAS: full analysis set, PPS: per-protocol set.
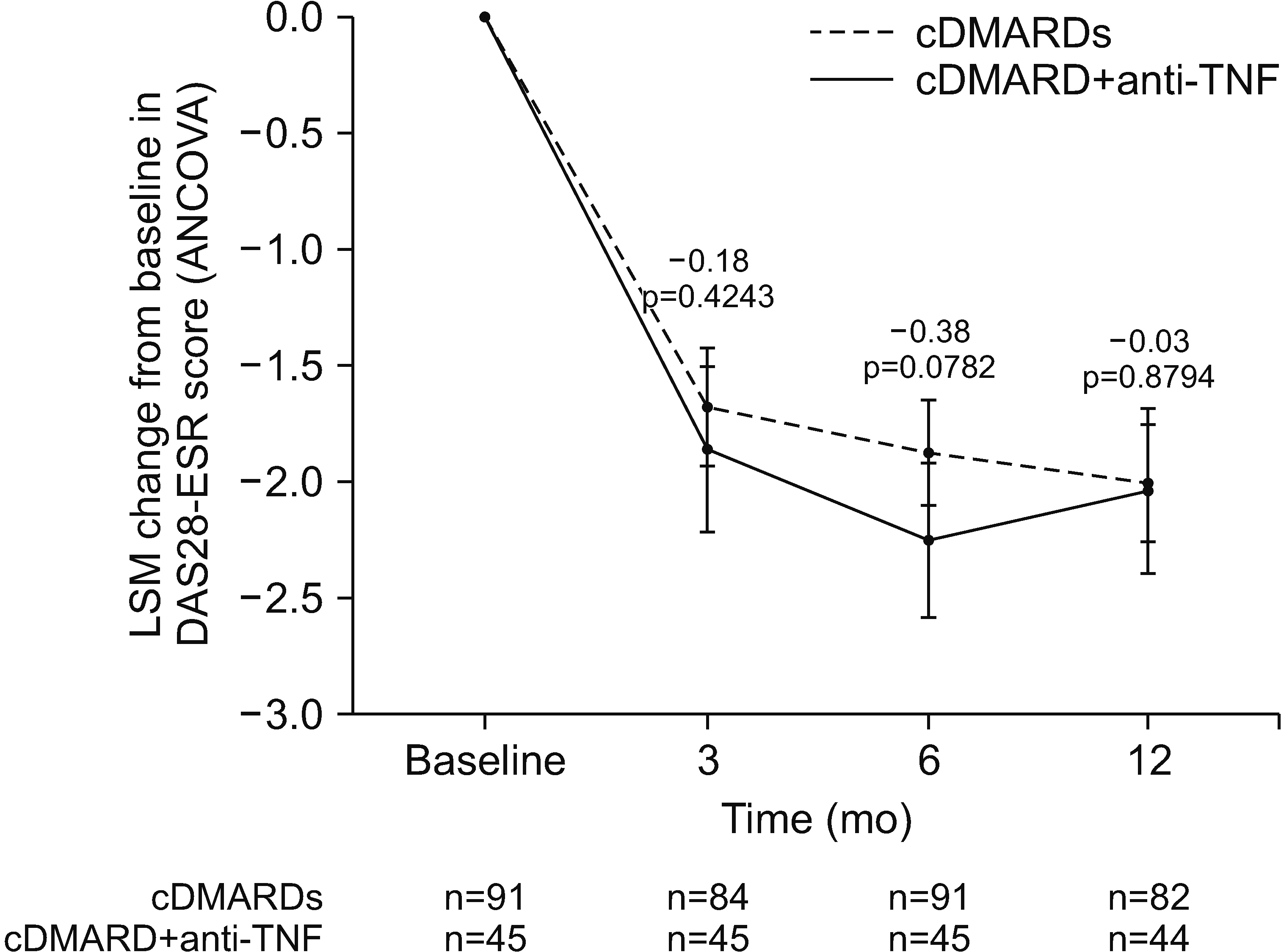
Figure 2 Change from baseline in disease activity score 28-joint count with erythrocyte sedimentation rate (DAS28-ESR) scores at 3, 6, and 12 months (per-protocol set). Results of ANCOVA of LSMs using patient age, duration of rheumatoid arthritis, and baseline DAS28-ESR score as covariates. Bars indicate 95% confidence intervals for each treatment group. Values above bars indicate the difference between the cDMARD+anti-TNF and cDMARDs groups. Baseline mean DAS28-ESR scores were 5.62 points in the points in the cDMARD+anti-TNF group vs 4.77 points in the multiple cDMARD group (p<0.001). ANCOVA: analysis of covariance, anti-TNF: anti-tumor necrosis factor agent, cDMARD: conventional disease-modifying anti-rheumatic drug, LSM: least square.
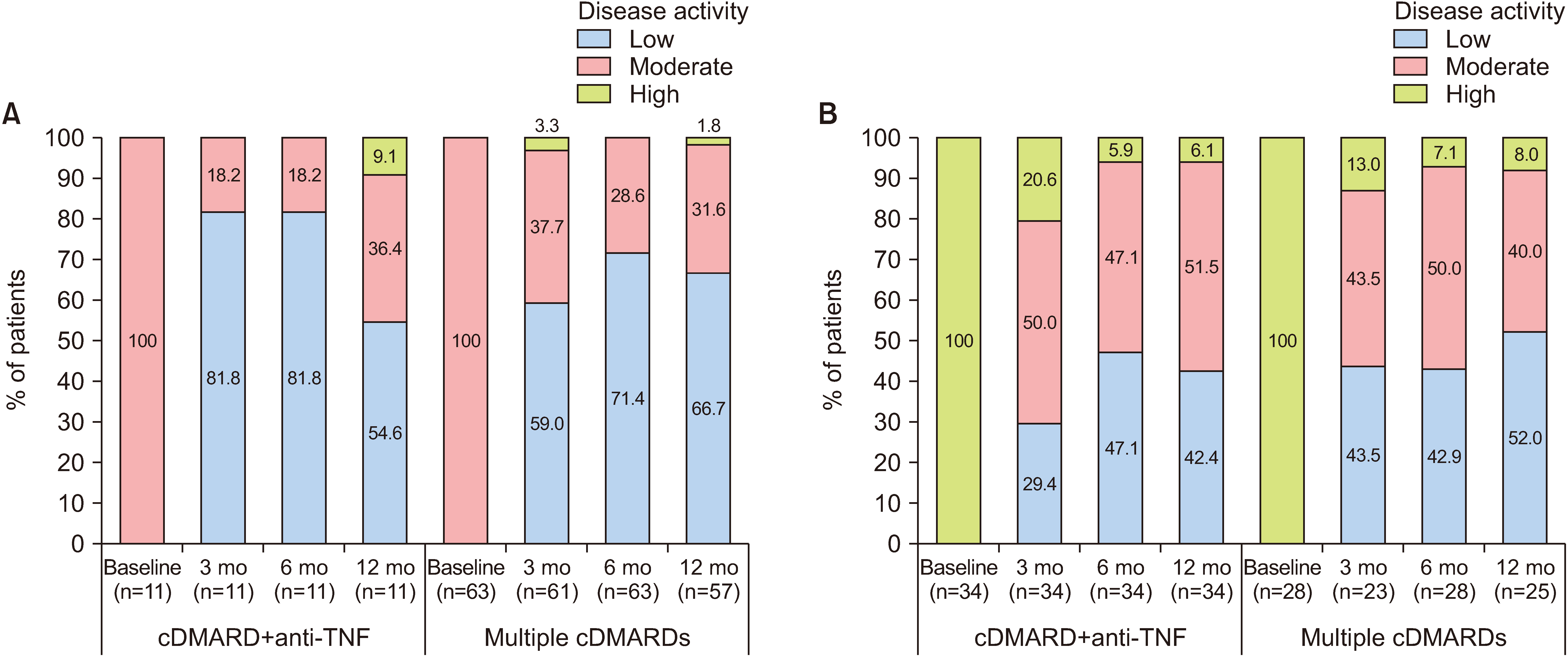
Figure 3 Effect of treatment on baseline disease activity status (per-protocol set). Proportion of patients with low, moderate or high disease activity at months 3, 6, and 12 in patients with (A) moderate disease activity at baseline, and (B) high disease activity at baseline. Based on European League Against Rheumatism (EULAR) response criteria, disease activity was classified as low (DAS28-ESR ≤3.2), moderate (DAS28-ESR >3.2 to ≤5.1) or high (DAS28-ESR >5.1) at baseline, then reclassified at each timepoint. There were no significant between-group differences in disease activity status at any timepoint. Anti-TNF: anti-tumor necrosis factor agent, cDMARD: conventional disease-modifying anti-rheumatic drug, DAS28-ESR: disease activity score 28-joint count with erythrocyte sedimentation rate.
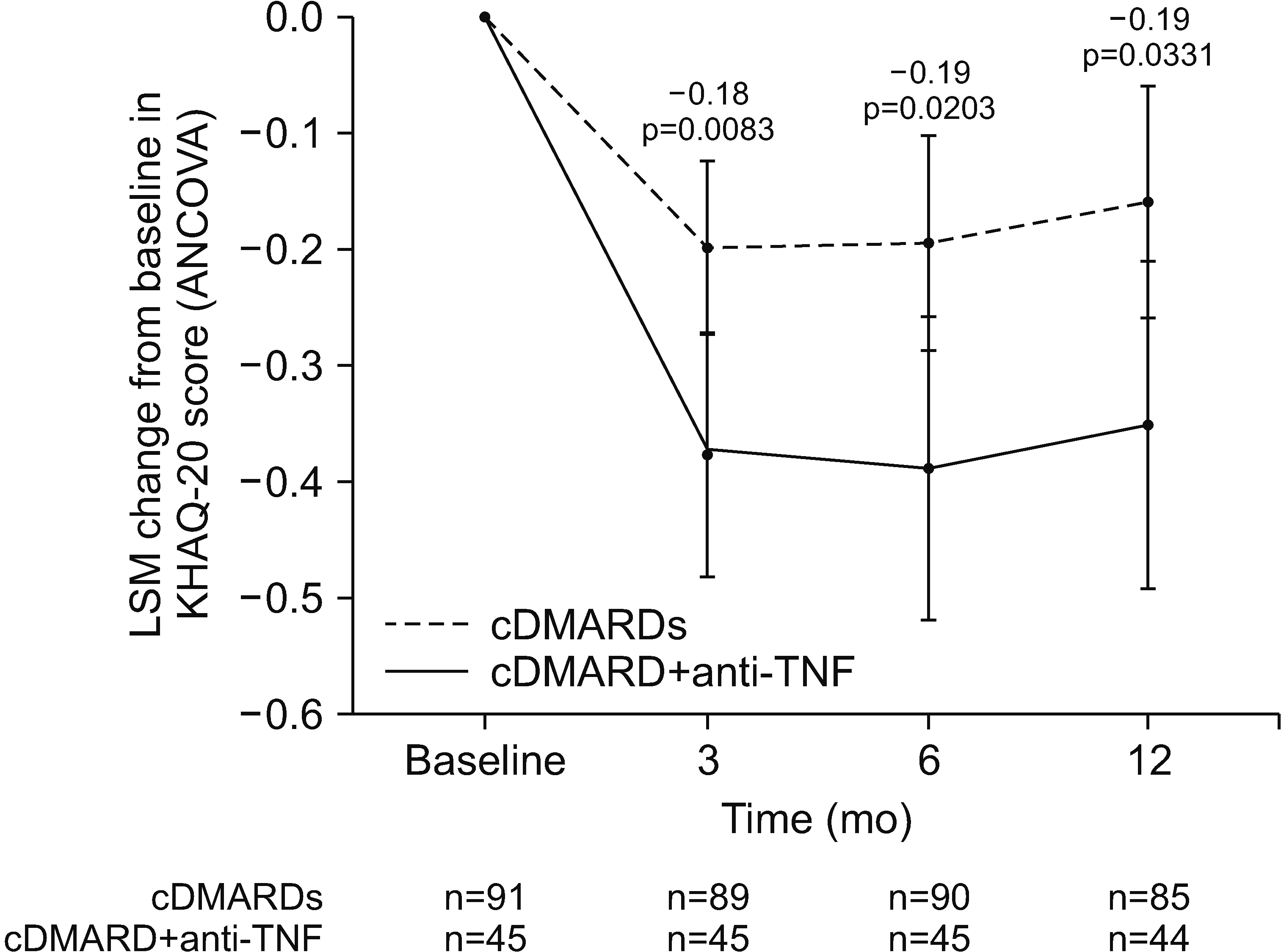
Figure 4 Change from baseline in quality-of-life, as measured by KHAQ-20 scores, at 3, 6, and 12 months (per-protocol set). Results of ANCOVA of LSMs means using patient age, duration of rheumatoid arthritis, and baseline KHAQ-20 scores as covariates. Bars indicate 95% confidence intervals for each treatment group. Values above bars indicate the difference between the cDMARD+anti-TNF and cDMARDs groups. Baseline mean KHAQ-20 scores were 0.95 points in the cDMARD+anti-TNF group vs 0.59 points in multiple cDMARD group (p=0.013). ANCOVA: analysis of covariance, anti-TNF: anti-tumor necrosis factor agent, cDMARD: conventional disease-modifying anti-rheumatic drug, KHAQ: Korean Health Assessment Questionnaire, LSM: least square mean.
Reference
-
1. Calabresi E, Petrelli F, Bonifacio AF, Puxeddu I, Alunno A. 2018; One year in review 2018: pathogenesis of rheumatoid arthritis. Clin Exp Rheumatol. 36:175–84.2. Won S, Cho SK, Kim D, Han M, Lee J, Jang EJ, et al. 2018; Update on the prevalence and incidence of rheumatoid arthritis in Korea and an analysis of medical care and drug utilization. Rheumatol Int. 38:649–56. DOI: 10.1007/s00296-017-3925-9. PMID: 29302803.
Article3. Fraenkel L, Bathon JM, England BR, St Clair EW, Arayssi T, Carandang K, et al. 2021; 2021 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Care Res (Hoboken). 73:924–39. DOI: 10.1002/acr.24596. PMID: 34101387. PMCID: PMC9273041.
Article4. Smolen JS, Landewé RBM, Bergstra SA, Kerschbaumer A, Sepriano A, Aletaha D, et al. 2023; EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 82:3–18. Erratum in: Ann Rheum Dis 2023;82:e76. DOI: 10.1136/ard-2022-223356corr1. PMID: 36764818.5. 2021. Jul. 6. Xeljanz (tofacitinib): increased risk of major adverse cardiovascular events and malignancies with use of tofacitinib relative to TNF-alpha inhibitors [Internet]. European Medicines Agency;Amsterdam: Available from: https://www.ema.europa.eu/en/medicines/dhpc/xeljanz-tofacitinib-increased-risk-major-adverse-cardiovascular-events-malignancies-use-tofacitinib. cited 2023 Jul 5.6. Ma MH, Kingsley GH, Scott DL. 2010; A systematic comparison of combination DMARD therapy and tumour necrosis inhibitor therapy with methotrexate in patients with early rheumatoid arthritis. Rheumatology (Oxford). 49:91–8. DOI: 10.1093/rheumatology/kep331. PMID: 19917618.
Article7. Graudal N, Hubeck-Graudal T, Faurschou M, Baslund B, Jürgens G. 2015; Combination therapy with and without tumor necrosis factor inhibitors in rheumatoid arthritis: a meta-analysis of randomized trials. Arthritis Care Res (Hoboken). 67:1487–95. DOI: 10.1002/acr.22618. PMID: 25989246.
Article8. Graudal N, Hubeck-Graudal T, Tarp S, Christensen R, Jürgens G. 2014; Effect of combination therapy on joint destruction in rheumatoid arthritis: a network meta-analysis of randomized controlled trials. PLoS One. 9:e106408. DOI: 10.1371/journal.pone.0106408. PMID: 25244021. PMCID: PMC4171366.
Article9. Curtis JR, Palmer JL, Reed GW, Greenberg J, Pappas DA, Harrold LR, et al. 2021; Real-world outcomes associated with methotrexate, sulfasalazine, and hydroxychloroquine triple therapy versus tumor necrosis factor inhibitor/methotrexate combination therapy in patients with rheumatoid arthritis. Arthritis Care Res (Hoboken). 73:1114–24. DOI: 10.1002/acr.24253. PMID: 32374918.
Article10. Bergstra SA, Winchow LL, Murphy E, Chopra A, Salomon-Escoto K, Fonseca JE, et al. 2019; How to treat patients with rheumatoid arthritis when methotrexate has failed? The use of a multiple propensity score to adjust for confounding by indication in observational studies. Ann Rheum Dis. 78:25–30. DOI: 10.1136/annrheumdis-2018-213731. PMID: 30327328.
Article11. van Gestel AM, Prevoo ML, van Rijswijk MH, van de Putte LB, van Riel PL. van 't Hof MA. 1996; Development and validation of the European League Against Rheumatism response criteria for rheumatoid arthritis. Comparison with the preliminary American College of Rheumatology and the World Health Organization/International League Against Rheumatism Criteria. Arthritis Rheum. 39:34–40. DOI: 10.1002/art.1780390105. PMID: 8546736.
Article12. Nishimoto N, Takagi N. 2010; Assessment of the validity of the 28-joint disease activity score using erythrocyte sedimentation rate (DAS28-ESR) as a disease activity index of rheumatoid arthritis in the efficacy evaluation of 24-week treatment with tocilizumab: subanalysis of the SATORI study. Mod Rheumatol. 20:539–47. DOI: 10.3109/s10165-010-0328-0. PMID: 20617358. PMCID: PMC2999727.
Article13. Fransen J, van Riel PL. 2009; The Disease Activity Score and the EULAR response criteria. Rheum Dis Clin North Am. 35:745–57. vii–viii. DOI: 10.1016/j.rdc.2009.10.001. PMID: 19962619.
Article14. Kavanaugh A, Fleischmann RM, Emery P, Kupper H, Redden L, Guerette B, et al. 2013; Clinical, functional and radiographic consequences of achieving stable low disease activity and remission with adalimumab plus methotrexate or methotrexate alone in early rheumatoid arthritis: 26-week results from the randomised, controlled OPTIMA study. Ann Rheum Dis. 72:64–71. DOI: 10.1136/annrheumdis-2011-201247. PMID: 22562973. PMCID: PMC3551224.
Article15. Kay J, Matteson EL, Dasgupta B, Nash P, Durez P, Hall S, et al. 2008; Golimumab in patients with active rheumatoid arthritis despite treatment with methotrexate: a randomized, double-blind, placebo-controlled, dose-ranging study. Arthritis Rheum. 58:964–75. Erratum in: Arthritis Rheum 2010;62:3518. DOI: 10.1002/art.23383. PMID: 18383539.
Article16. Atzeni F, Talotta R, Salaffi F, Cassinotti A, Varisco V, Battellino M, et al. 2013; Immunogenicity and autoimmunity during anti-TNF therapy. Autoimmun Rev. 12:703–8. DOI: 10.1016/j.autrev.2012.10.021. PMID: 23207283.
Article17. Anderson PJ. 2005; Tumor necrosis factor inhibitors: clinical implications of their different immunogenicity profiles. Semin Arthritis Rheum. 34(5 Suppl 1):19–22. DOI: 10.1016/j.semarthrit.2005.01.005. PMID: 15852250.
Article18. Sode J, Vogel U, Bank S, Andersen PS, Hetland ML, Locht H, et al. 2018; Confirmation of an IRAK3 polymorphism as a genetic marker predicting response to anti-TNF treatment in rheumatoid arthritis. Pharmacogenomics J. 18:81–6. DOI: 10.1038/tpj.2016.66. PMID: 27698401.
Article19. Scott DL, Ibrahim F, Farewell V, O'Keeffe AG, Walker D, Kelly C, et al. 2015; Tumour necrosis factor inhibitors versus combination intensive therapy with conventional disease modifying anti-rheumatic drugs in established rheumatoid arthritis: TACIT non-inferiority randomised controlled trial. BMJ. 350:h1046. DOI: 10.1136/bmj.h1046. PMID: 25769495. PMCID: PMC4358851.
Article20. Berardicurti O, Ruscitti P, Pavlych V, Conforti A, Giacomelli R, Cipriani P. 2020; Glucocorticoids in rheumatoid arthritis: the silent companion in the therapeutic strategy. Expert Rev Clin Pharmacol. 13:593–604. DOI: 10.1080/17512433.2020.1772055. PMID: 32434398.
Article21. Hua C, Buttgereit F, Combe B. 2020; Glucocorticoids in rheumatoid arthritis: current status and future studies. RMD Open. 6:e000536. DOI: 10.1136/rmdopen-2017-000536. PMID: 31958273. PMCID: PMC7046968.
Article22. Pope JE, Khanna D, Norrie D, Ouimet JM. 2009; The minimally important difference for the health assessment questionnaire in rheumatoid arthritis clinical practice is smaller than in randomized controlled trials. J Rheumatol. 36:254–9. DOI: 10.3899/jrheum.080479. PMID: 19132791.
Article23. Cho SK, Bae SC. 2017; Pharmacologic treatment of rheumatoid arthritis. J Korean Med Assoc. 60:156–63. DOI: 10.5124/jkma.2017.60.2.156.
Article24. Heckman MG, Davis JM 3rd, Crowson CS. 2022; Post hoc power calculations: an inappropriate method for interpreting the findings of a research study. J Rheumatol. 49:867–70. DOI: 10.3899/jrheum.211115. PMID: 35105710.
Article25. Fraser RA. 2023; Inappropriate use of statistical power. Bone Marrow Transplant. 58:474–7. DOI: 10.1038/s41409-023-01935-3. PMID: 36869191.
Article26. Giacomelli R, Afeltra A, Bartoloni E, Berardicurti O, Bombardieri M, Bortoluzzi A, et al. 2021; The growing role of precision medicine for the treatment of autoimmune diseases; results of a systematic review of literature and Experts' Consensus. Autoimmun Rev. 20:102738. DOI: 10.1016/j.autrev.2020.102738. PMID: 33326854.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrent Pneumothorax after Etanercept Therapy in a Rheumatoid Arthritis Patient: A Case Report
- Persistence with Anti-TNF Therapies in Patients with Rheumatoid Arthritis
- Comparative Effectiveness of Biologic DMARDs in Rheumatoid Arthritis Patients with Inadequate Response to conventional DMARDs: Using a Bayesian Network Meta-analysis
- Update on rheumatoid arthritis
- Diagnostic Signification of Antiperinuclear Factor(APF) in Rheumatoid Arthritis
