Korean J Gastroenterol.
2023 Jul;82(1):25-29. 10.4166/kjg.2023.056.
Immunoglobulin G4-related Disease of the Small Bowel: A Case of Long-term Remission Achieved by Surgical Resection without Maintenance Therapy
- Affiliations
-
- 1Departments of Internal Medicine, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea
- 2Departments of Pathology, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea
- KMID: 2544936
- DOI: http://doi.org/10.4166/kjg.2023.056
Abstract
- Immunoglobulin G4-related disease (IgG4-RD) is an immune-mediated fibroinflammatory disease. IgG4-RD can affect any organ system, including the pancreas, bile ducts, salivary glands, mesentery, and retroperitoneum. On the other hand, small intestine involvement is extremely rare. This paper describes a case of IgG4-RD involving the small bowel, particularly at the distal ileum. An 81-year-old female was admitted to the authors’ hospital complaining of abdominal pain, dyspepsia, and hematochezia. The laboratory tests, including tumor markers and IgG4, were within normal limits. A colonoscopy did not show any abnormal findings. Abdominal computed tomography revealed segmental aneurysmal dilatation and wall thickening at the distal ileum, suggesting malignant conditions, such as small bowel lymphoma. The patient underwent an exploratory laparoscopy and ileocecectomy to differentiate a malignancy. A histopathology examination revealed dense lymphoplasmacytic infiltration, storiform fibrosis, and IgG4-positive plasma cells (>50 per high power field). The patient was finally diagnosed with IgG4-RD. The patient was followed up in the outpatient clinic for five years without recurrence. This paper suggests that a radical resection without maintenance therapy can be a treatment option, particularly when the IgG4-RD manifests as a localized gastrointestinal tract lesion.
Keyword
Figure
-
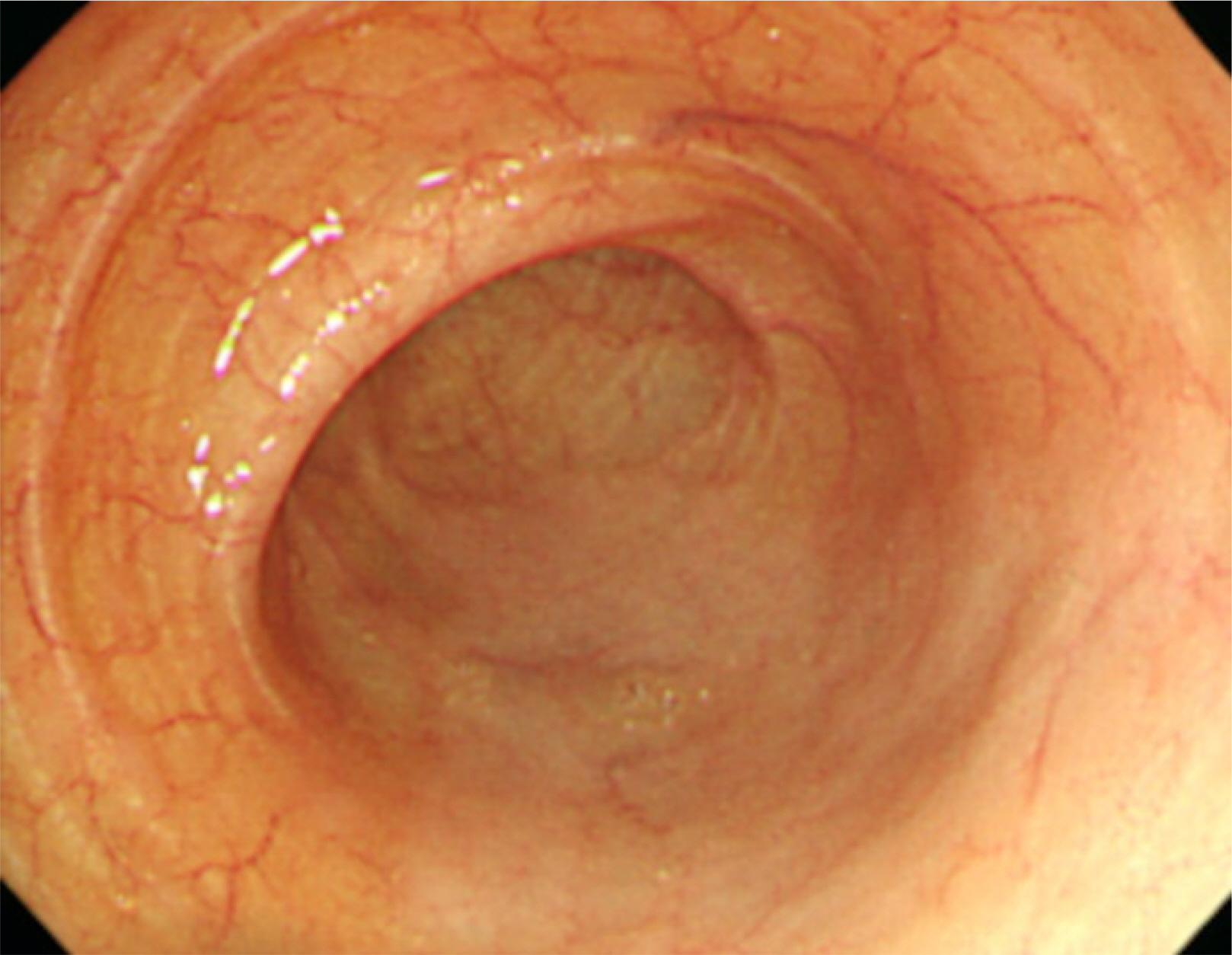
Fig. 1 Colonoscopy shows the normal findings of the terminal ileum.
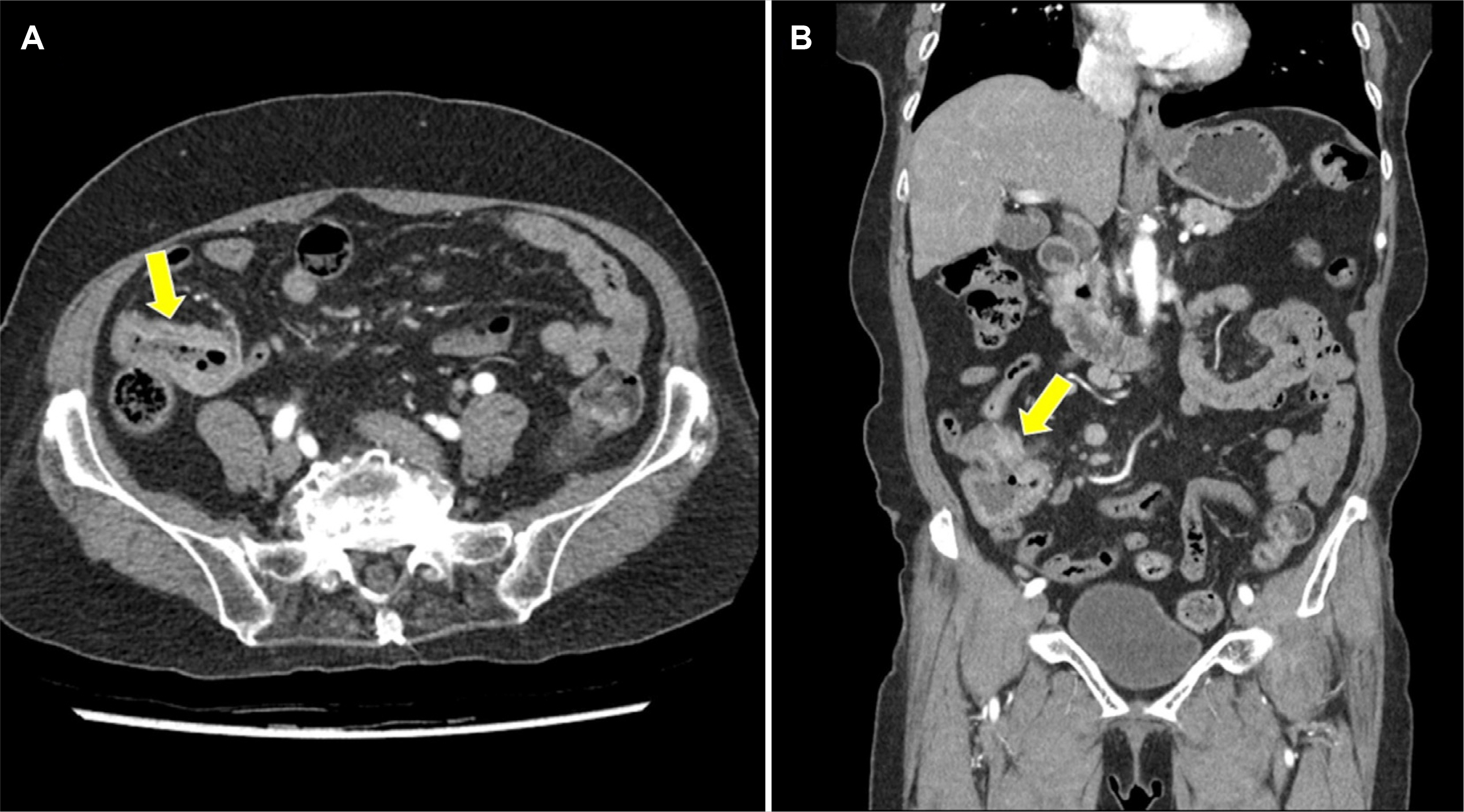
Fig. 2 Abdominal computed tomography shows segmental aneurysmal dilatation and wall thickening at the distal ileum (arrow) on axial (A) and coronal view (B).
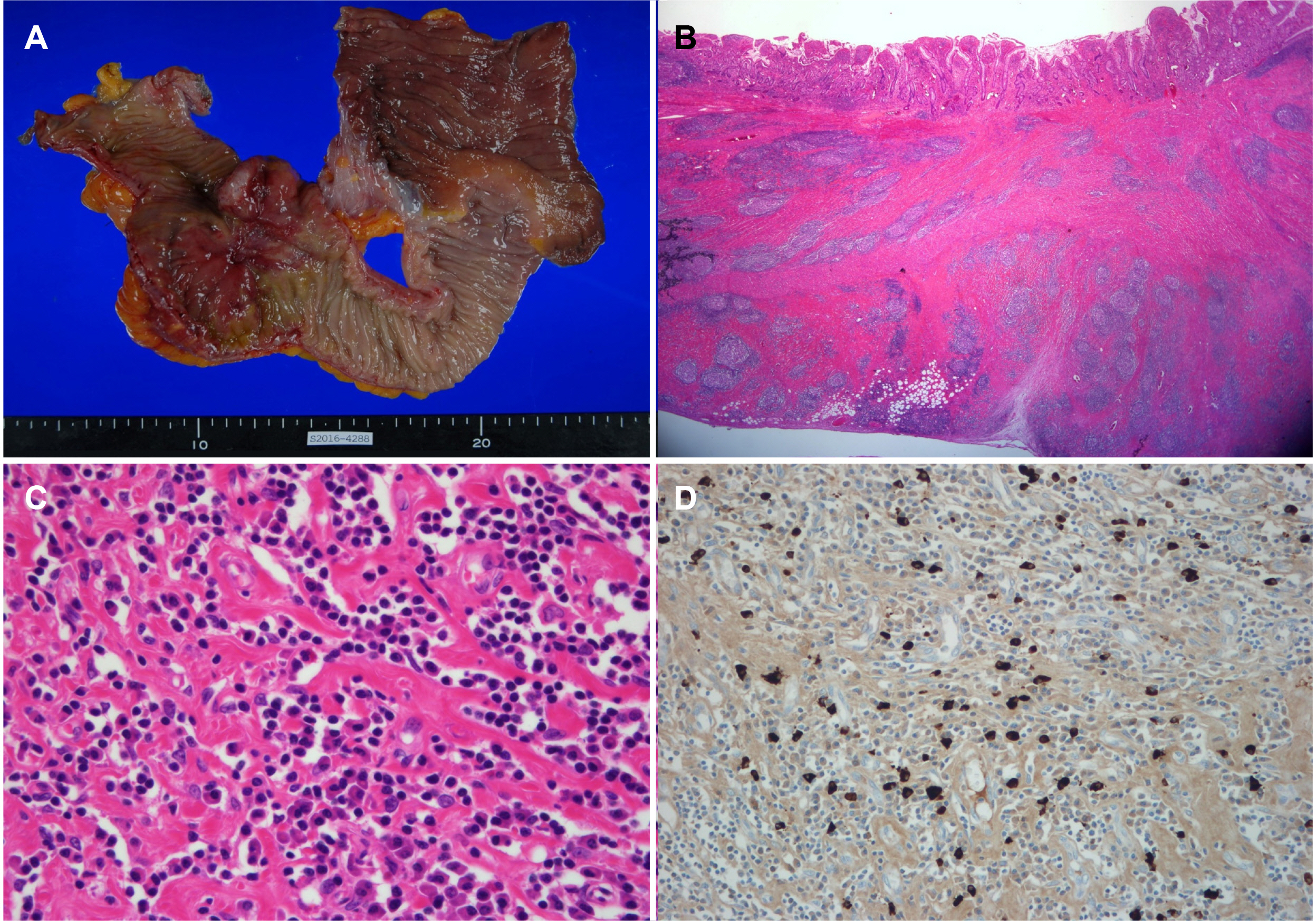
Fig. 3 (A) Gross specimen from segmental bowel resection shows a huge ulceroinfiltrative lesion at the distal ileum. (B) Pathologic findings with a low magnification view reveal transmural inflammation with many lymphoid follicles and sclerotic fibrosis (H&E, ×10). (C) Inflammatory infiltrates predominantly comprise plasma cells, lymphocytes, and some eosinophils (H&E, ×200). (D) Immunohistochemical stain reveals many IgG4-positive cells with more than 50 cells per high power field (×200).
Reference
-
1. Löhr JM, Vujasinovic M, Rosendahl J, Stone JH, Beuers U. 2022; IgG4-related diseases of the digestive tract. Nat Rev Gastroenterol Hepatol. 19:185–197. DOI: 10.1038/s41575-021-00529-y. PMID: 34750548.2. Lee YS, Lee SH, Lee MG, et al. 2013; Immunoglobulin g4-related disease mimicking unresectable gallbladder cancer. Gut Liver. 7:616–620. DOI: 10.5009/gnl.2013.7.5.616. PMID: 24073322. PMCID: PMC3782679.3. Moon SH, Kim MH. 2022; Autoimmune pancreatitis and immunoglobulin G4-related sclerosing cholangitis: Past, present, and future. Korean J Gastroenterol. 80:107–114. DOI: 10.4166/kjg.2022.102. PMID: 36156034.4. Umehara H, Okazaki K, Kawa S, et al. 2021; The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD. Mod Rheumatol. 31:529–533. DOI: 10.1080/14397595.2020.1859710. PMID: 33274670.5. Wallace ZS, Naden RP, Chari S, et al. 2020; The 2019 American College of Rheumatology/European League Against Rheumatism Classification Criteria for IgG4-related disease. Arthritis Rheumatol. 72:7–19. DOI: 10.1002/art.41120. PMID: 31793250.6. Umehara H, Okazaki K, Nakamura T, et al. 2017; Current approach to the diagnosis of IgG4-related disease - Combination of comprehensive diagnostic and organ-specific criteria. Mod Rheumatol. 27:381–391. DOI: 10.1080/14397595.2017.1290911. PMID: 28165852.7. Löhr JM, Beuers U, Vujasinovic M, et al. 2020; European Guideline on IgG4-related digestive disease - UEG and SGF evidence-based recommendations. United European Gastroenterol J. 8:637–666. DOI: 10.1177/2050640620934911. PMID: 32552502. PMCID: PMC7437085.8. Watanabe A, Goto T, Kamo H, et al. 2018; Resection of lesions in the ileum of patients with IgG4-related disease may ameliorate disease progression without steroid administration. Surg Case Rep. 4:148. DOI: 10.1186/s40792-018-0546-9. PMID: 30594958. PMCID: PMC6311175.9. Lee HW, Moon SH, Kim MH, et al. 2018; Relapse rate and predictors of relapse in a large single center cohort of type 1 autoimmune pancreatitis: long-term follow-up results after steroid therapy with short-duration maintenance treatment. J Gastroenterol. 53:967–977. DOI: 10.1007/s00535-018-1434-6. PMID: 29362937.10. Shiokawa M, Kodama Y, Yoshimura K, et al. 2013; Risk of cancer in patients with autoimmune pancreatitis. Am J Gastroenterol. 108:610–617. DOI: 10.1038/ajg.2012.465. PMID: 23318486.11. Hart PA, Law RJ, Dierkhising RA, Smyrk TC, Takahashi N, Chari ST. 2014; Risk of cancer in autoimmune pancreatitis: a case-control study and review of the literature. Pancreas. 43:417–421. DOI: 10.1097/MPA.0000000000000053. PMID: 24622072.12. Lee KW, Chang JH, Kim J, et al. 2020; Metachronous development of peritoneal carcinomatosis in a patient with autoimmune pancreatitis. Korean J Gastroenterol. 75:356–361. DOI: 10.4166/kjg.2020.75.6.356. PMID: 32581208.13. Wong DD, Pillai SR, Kumarasinghe MP, et al. 2012; IgG4-related sclerosing disease of the small bowel presenting as necrotizing mesenteric arteritis and a solitary jejunal ulcer. Am J Surg Pathol. 36:929–934. DOI: 10.1097/PAS.0b013e3182495c96. PMID: 22367294.14. Ko Y, Woo JY, Kim JW, et al. 2013; An immunoglobulin G4-related sclerosing disease of the small bowel: CT and small bowel series findings. Korean J Radiol. 14:776–780. DOI: 10.3348/kjr.2013.14.5.776. PMID: 24043971. PMCID: PMC3772257.15. Ciccone F, Ciccone A, Di Ruscio M, et al. 2018; IgG4-related disease mimicking Crohn's disease: A case report and review of literature. Dig Dis Sci. 63:1072–1086. DOI: 10.1007/s10620-018-4950-6. PMID: 29417330.16. Campos-Murguía A, Martinez-Garcia CL, Chable-Montero F, Zamora-Nava LE. 2023; Multifocal ulcerating stenosing enteritis as a novel manifestation of immunoglobulin G4-related disease. Endoscopy. 55(S 01):E163–E164. DOI: 10.1055/a-1952-0490. PMID: 36307068. PMCID: PMC9829813.17. Fujita K, Naganuma M, Saito E, et al. 2012; Histologically confirmed IgG4-related small intestinal lesions diagnosed via double balloon enteroscopy. Dig Dis Sci. 57:3303–3306. DOI: 10.1007/s10620-012-2267-4. PMID: 22695887.18. Hiyoshi Y, Oki E, Zaitsu Y, et al. 2014; IgG4-related disease of the ileocecal region mimicking malignancy: A case report. Int J Surg Case Rep. 5:669–672. DOI: 10.1016/j.ijscr.2014.08.003. PMID: 25194601. PMCID: PMC4189076.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Recurrent Ischemic Stroke Associated with Immunoglobulin G4-Related Disease
- Immunoglobulin G4-related sclerosing cholangitis
- De-escalation of Therapy in Patients with Quiescent Inflammatory Bowel Disease
- An Immunoglobulin G4-Related Sclerosing Disease of the Small Bowel: CT and Small Bowel Series Findings
- Anesthetic Management of Small Bowel Transplantation for Short Bowel Syndrome: A case report
