J Gastric Cancer.
2019 Mar;19(1):72-82. 10.5230/jgc.2019.19.e3.
Implementation of Enhanced Recovery after Surgery (ERAS) Program in Perioperative Management of Gastric Cancer Surgery: a Nationwide Survey in Korea
- Affiliations
-
- 1Division of Gastroenterologic Surgery, Department of Surgery, Chonnam National University Medical School, Gwangju, Korea. dr4477@hanmail.net
- KMID: 2458819
- DOI: http://doi.org/10.5230/jgc.2019.19.e3
Abstract
- PURPOSE
Despite its clinical benefits, enhanced recovery after surgery (ERAS) is less widely implemented for gastric cancer surgery. This nationwide survey investigated the current status of the implementation of ERAS in perioperative care for gastric cancer surgery in South Korea.
MATERIALS AND METHODS
This survey enrolled 89 gastric surgeons from 52 institutions in South Korea. The questionnaire consisted of 24 questions about the implementation of the ERAS protocols in the management of gastric cancer surgery. The survey was carried out using an electronic form sent via email.
RESULTS
Of the 89 gastric surgeons, 58 (65.2%) answered that they have knowledge of the concept and details of ERAS, 45 (50.6%) of whom were currently applying ERAS for their patients. Of the ERAS protocols, preoperative education (91.0%), avoidance of preoperative fasting (68.5%), maintenance of intraoperative normothermia (79.8%), thromboprophylaxis (96.5%), early active ambulation (64.4%), and early removal of urinary catheter (68.5%) were relatively well adopted in perioperative care. However, other practices, such as avoidance of preoperative bowel preparation (41.6%), provision of preoperative carbohydrate-rich drink (10.1%), avoidance of routine abdominal drainage (31.4%), epidural anesthesia (15.9%), single-dose prophylactic antibiotics (19.3%), postoperative high oxygen therapy (36.8%), early postoperative diet (14.6%), restricted intravenous fluid administration (53.9%), and application of discharge criteria (57.3%) were not very well adopted for patients.
CONCLUSIONS
Perioperative management of gastric cancer surgery is largely heterogeneous among gastric surgeons in South Korea. Standard perioperative care based on scientific evidence needs to be established to improve the quality of surgical care and patient outcomes.
MeSH Terms
Figure
-
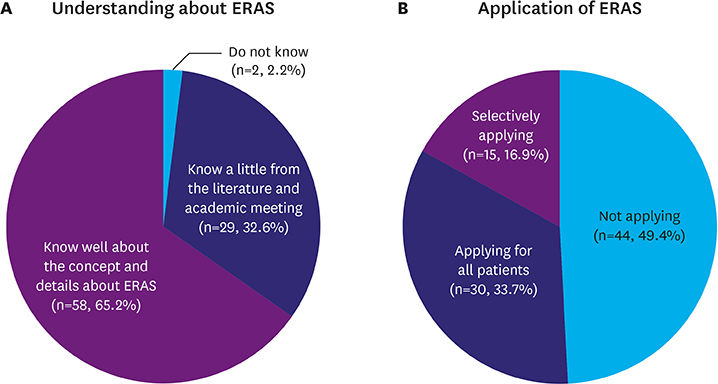
Fig. 1 Level of understanding about ERAS (A) and application of ERAS (B). ERAS = enhanced recovery after surgery.
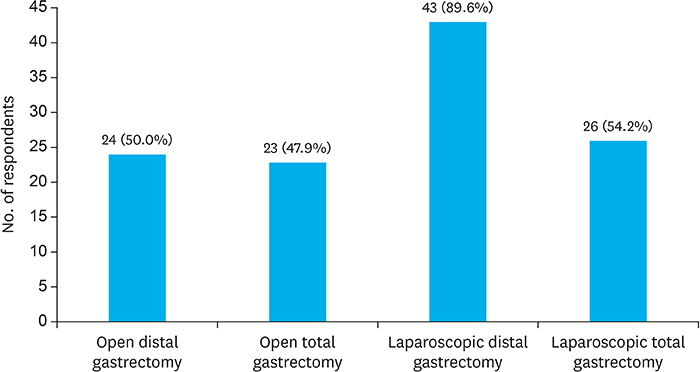
Fig. 2 Application of ERAS according to the type of operation. ERAS = enhanced recovery after surgery.
Cited by 1 articles
-
Challenging issues of implementing enhanced recovery after surgery programs in South Korea
Soo-Hyuk Yoon, Ho-Jin Lee
Anesth Pain Med. 2024;19(1):24-34. doi: 10.17085/apm.23096.
Reference
-
1. Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997; 78:606–617.
Article2. Varadhan KK, Neal KR, Dejong CH, Fearon KC, Ljungqvist O, Lobo DN. The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr. 2010; 29:434–440.
Article3. Teeuwen PH, Bleichrodt RP, Strik C, Groenewoud JJ, Brinkert W, van Laarhoven CJ, et al. Enhanced recovery after surgery (ERAS) versus conventional postoperative care in colorectal surgery. J Gastrointest Surg. 2010; 14:88–95.
Article4. King PM, Blazeby JM, Ewings P, Longman RJ, Kipling RM, Franks PJ, et al. The influence of an enhanced recovery programme on clinical outcomes, costs and quality of life after surgery for colorectal cancer. Colorectal Dis. 2006; 8:506–513.
Article5. Qi S, Chen G, Cao P, Hu J, He G, Luo J, et al. Safety and efficacy of enhanced recovery after surgery (ERAS) programs in patients undergoing hepatectomy: a prospective randomized controlled trial. J Clin Lab Anal. 2018; 32:e22434.
Article6. Takagi K, Yoshida R, Yagi T, Umeda Y, Nobuoka D, Kuise T, et al. Effect of an enhanced recovery after surgery protocol in patients undergoing pancreaticoduodenectomy: a randomized controlled trial. Clin Nutr. 2018; S0261-5614(18)30002-5.
Article7. Polle SW, Wind J, Fuhring JW, Hofland J, Gouma DJ, Bemelman WA. Implementation of a fast-track perioperative care program: what are the difficulties? Dig Surg. 2007; 24:441–449.
Article8. Maessen J, Dejong CH, Hausel J, Nygren J, Lassen K, Andersen J, et al. A protocol is not enough to implement an enhanced recovery programme for colorectal resection. Br J Surg. 2007; 94:224–231.
Article9. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017; 152:292–298.10. Gustafsson UO, Scott MJ, Schwenk W, Demartines N, Roulin D, Francis N, et al. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. World J Surg. 2013; 37:259–284.11. Lassen K, Coolsen MM, Slim K, Carli F, de Aguilar-Nascimento JE, Schäfer M, et al. Guidelines for perioperative care for pancreaticoduodenectomy: Enhanced Recovery After Surgery (ERAS®) Society recommendations. World J Surg. 2013; 37:240–258.12. Nygren J, Thorell A, Ljungqvist O. Preoperative oral carbohydrate nutrition: an update. Curr Opin Clin Nutr Metab Care. 2001; 4:255–259.
Article13. Mortensen K, Nilsson M, Slim K, Schäfer M, Mariette C, Braga M, et al. Consensus guidelines for enhanced recovery after gastrectomy: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Br J Surg. 2014; 101:1209–1229.14. Lemanu DP, Singh PP, Berridge K, Burr M, Birch C, Babor R, et al. Randomized clinical trial of enhanced recovery versus standard care after laparoscopic sleeve gastrectomy. Br J Surg. 2013; 100:482–489.
Article15. Kim JW, Kim WS, Cheong JH, Hyung WJ, Choi SH, Noh SH. Safety and efficacy of fast-track surgery in laparoscopic distal gastrectomy for gastric cancer: a randomized clinical trial. World J Surg. 2012; 36:2879–2887.
Article16. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2017; 20:1–19.17. Liu HP, Zhang YC, Zhang YL, Yin LN, Wang J. Drain versus no-drain after gastrectomy for patients with advanced gastric cancer: systematic review and meta-analysis. Dig Surg. 2011; 28:178–189.
Article18. Nelson R, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev. 2005; CD004929.
Article19. Yang Z, Zheng Q, Wang Z. Meta-analysis of the need for nasogastric or nasojejunal decompression after gastrectomy for gastric cancer. Br J Surg. 2008; 95:809–816.
Article20. Holte K, Nielsen KG, Madsen JL, Kehlet H. Physiologic effects of bowel preparation. Dis Colon Rectum. 2004; 47:1397–1402.
Article21. Zaouter C, Kaneva P, Carli F. Less urinary tract infection by earlier removal of bladder catheter in surgical patients receiving thoracic epidural analgesia. Reg Anesth Pain Med. 2009; 34:542–548.
Article22. Benoist S, Panis Y, Denet C, Mauvais F, Mariani P, Valleur P. Optimal duration of urinary drainage after rectal resection: a randomized controlled trial. Surgery. 1999; 125:135–141.
Article23. Ljungqvist O, Søreide E. Preoperative fasting. Br J Surg. 2003; 90:400–406.
Article24. American Society of Anesthesiologists Committee. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters. Anesthesiology. 2011; 114:495–511.25. Svanfeldt M, Thorell A, Hausel J, Soop M, Rooyackers O, Nygren J, et al. Randomized clinical trial of the effect of preoperative oral carbohydrate treatment on postoperative whole-body protein and glucose kinetics. Br J Surg. 2007; 94:1342–1350.
Article26. Kurz A, Sessler DI, Lenhardt R. Study of Wound Infection and Temperature Group. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. N Engl J Med. 1996; 334:1209–1215.
Article27. Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg. 2002; 183:630–641.
Article28. Lewis SJ, Egger M, Sylvester PA, Thomas S. Early enteral feeding versus “nil by mouth” after gastrointestinal surgery: systematic review and meta-analysis of controlled trials. BMJ. 2001; 323:773–776.
Article29. Andersen HK, Lewis SJ, Thomas S. Early enteral nutrition within 24h of colorectal surgery versus later commencement of feeding for postoperative complications. Cochrane Database Syst Rev. 2006; CD004080.
Article30. Soop M, Carlson GL, Hopkinson J, Clarke S, Thorell A, Nygren J, et al. Randomized clinical trial of the effects of immediate enteral nutrition on metabolic responses to major colorectal surgery in an enhanced recovery protocol. Br J Surg. 2004; 91:1138–1145.
Article31. Charoenkwan K, Phillipson G, Vutyavanich T. Early versus delayed (traditional) oral fluids and food for reducing complications after major abdominal gynaecologic surgery. Cochrane Database Syst Rev. 2007; CD004508.
Article32. Lobo DN, Bostock KA, Neal KR, Perkins AC, Rowlands BJ, Allison SP. Effect of salt and water balance on recovery of gastrointestinal function after elective colonic resection: a randomised controlled trial. Lancet. 2002; 359:1812–1818.
Article33. Holte K, Sharrock NE, Kehlet H. Pathophysiology and clinical implications of perioperative fluid excess. Br J Anaesth. 2002; 89:622–632.
Article34. MacKay G, Fearon K, McConnachie A, Serpell MG, Molloy RG, O'Dwyer PJ. Randomized clinical trial of the effect of postoperative intravenous fluid restriction on recovery after elective colorectal surgery. Br J Surg. 2006; 93:1469–1474.
Article35. Brandstrup B, Tønnesen H, Beier-Holgersen R, Hjortsø E, Ørding H, Lindorff-Larsen K, et al. Effects of intravenous fluid restriction on postoperative complications: comparison of two perioperative fluid regimens: a randomized assessor-blinded multicenter trial. Ann Surg. 2003; 238:641–648.36. Gan TJ, Soppitt A, Maroof M, el-Moalem H, Robertson KM, Moretti E, et al. Goal-directed intraoperative fluid administration reduces length of hospital stay after major surgery. Anesthesiology. 2002; 97:820–826.
Article37. Conway DH, Mayall R, Abdul-Latif MS, Gilligan S, Tackaberry C. Randomised controlled trial investigating the influence of intravenous fluid titration using oesophageal Doppler monitoring during bowel surgery. Anaesthesia. 2002; 57:845–849.
Article38. Marret E, Remy C, Bonnet F. Postoperative Pain Forum Group. Meta-analysis of epidural analgesia versus parenteral opioid analgesia after colorectal surgery. Br J Surg. 2007; 94:665–673.
Article39. Zutshi M, Delaney CP, Senagore AJ, Mekhail N, Lewis B, Connor JT, et al. Randomized controlled trial comparing the controlled rehabilitation with early ambulation and diet pathway versus the controlled rehabilitation with early ambulation and diet with preemptive epidural anesthesia/analgesia after laparotomy and intestinal resection. Am J Surg. 2005; 189:268–272.
Article40. Rigg JR, Jamrozik K, Myles PS, Silbert BS, Peyton PJ, Parsons RW, et al. Epidural anaesthesia and analgesia and outcome of major surgery: a randomised trial. Lancet. 2002; 359:1276–1282.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Enhanced recovery after surgery: anesthesia-related components
- Which patients with gastric cancer should be candidates for Enhanced Recovery After Surgery protocols?
- Perception and implementation status of enhanced recovery after surgery
- Challenging issues of implementing enhanced recovery after surgery programs in South Korea
- Implementation of the enhanced recovery after surgery protocol for radical cystectomy patients: A single centre experience
