J Korean Ophthalmol Soc.
2008 Sep;49(9):1379-1386.
Pseudotumor : Distribution, Clinical Features, Treatment Outcomes
- Affiliations
-
- 1Myung-Gok Eye Research Institute, Department of Ophthalmology, Konyang University, Kim's Eye Hospital, Seoul, Korea. greatj@unitel.co.kr
- 2Department of Ophthalmology, Cheju National University, College of Medicine, Jeju, Korea.
Abstract
- PURPOSE
To evaluate the clinical characteristics and results of outcomes in different types of orbital pseudotumor.
METHODS
This study included 62 patients diagnosed with orbital pseudotumor between 2002 and 2007, who were followed-up for more than 6 months. The pseudotumor was classified into anterior, diffuse, apical, myositic, or lacrimal types according to computed tomography (CT) findings. All patients were initially treated with corticosteroids and checked for symptom improvement and response to the corticosteroids.
RESULTS
Lacrimal type pseudotumor (61%, 39/62) showed the highest incidence, and lid swelling (97%, 60/62) was the most common symptom. Response rate to corticosteroid treatment was 84%, and the recurrence rate was 29%.
CONCLUSIONS
The orbital pseudotumors were localized by computed tomography and classified to compare the symptoms, treatment efficacy and recurrence rates between the different types. The orbital pseudotumor is most commonly diagnosed based on clinical symptomsand radiologic features without biopsy. The orbital pseudotumor showed a good treatment response but also a high recurrence rate. Therefore, when starting treatment, it is important to consider differential diagnosis. It is recommended to carefully examine patients who have lid swelling for a few weeks with computed tomography before using corticosteroid treatment.
Keyword
MeSH Terms
Figure
-

Figure 1. Anterior type, CT image shows a ragged infiltration involvingthe anterior soft tissue of the right orbit and surrounding the right globe.
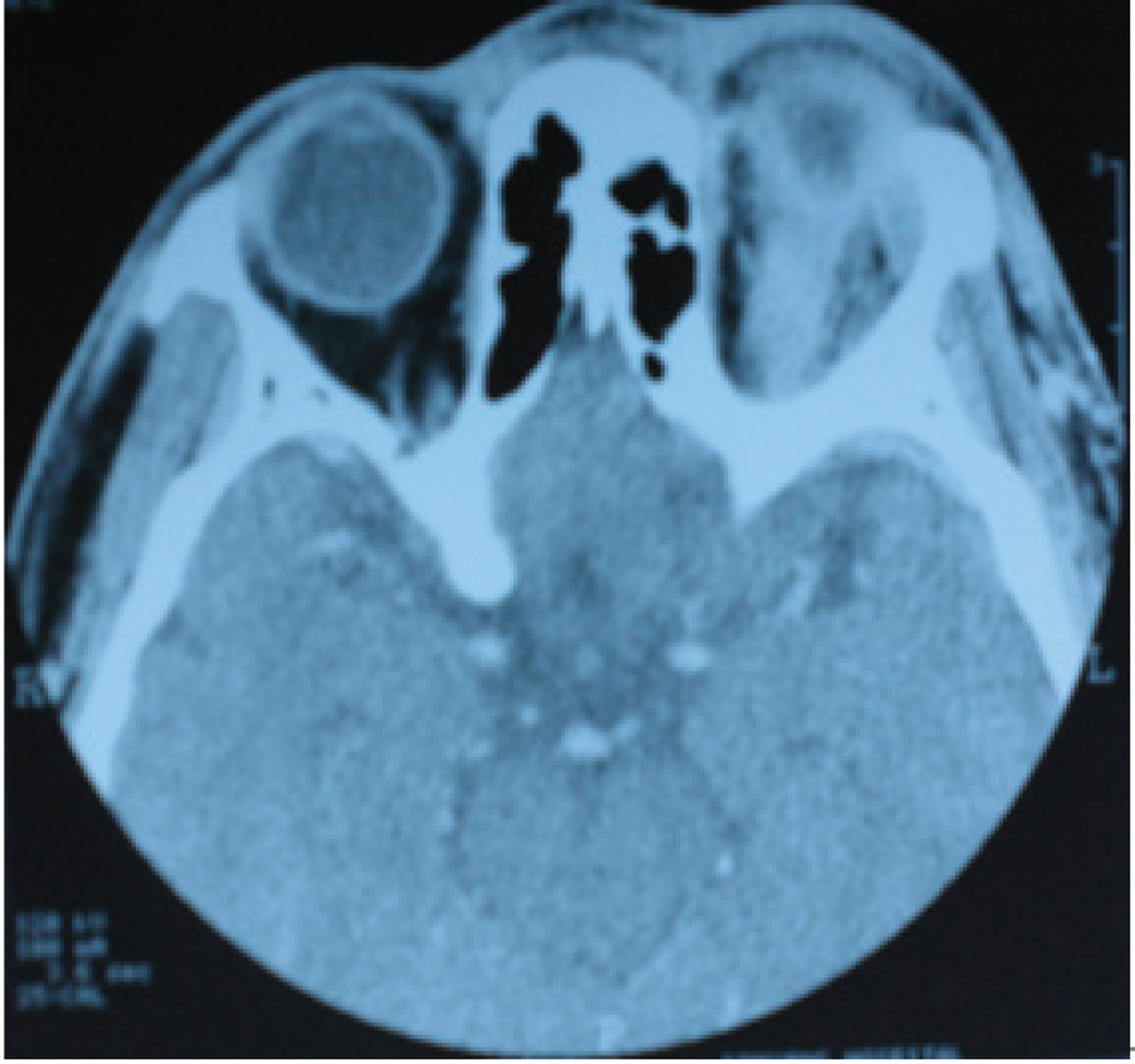
Figure 2. Diffuse type, CT scan shows soft tissue infiltration involving the entire orbit, extending from the apex to the posterior margin of the right globe.

Figure 3. Apical type, CT scan shows a mass of the apex of the right orbit with extension along the posterior portion of the extraocular muscles and the optic nerve.
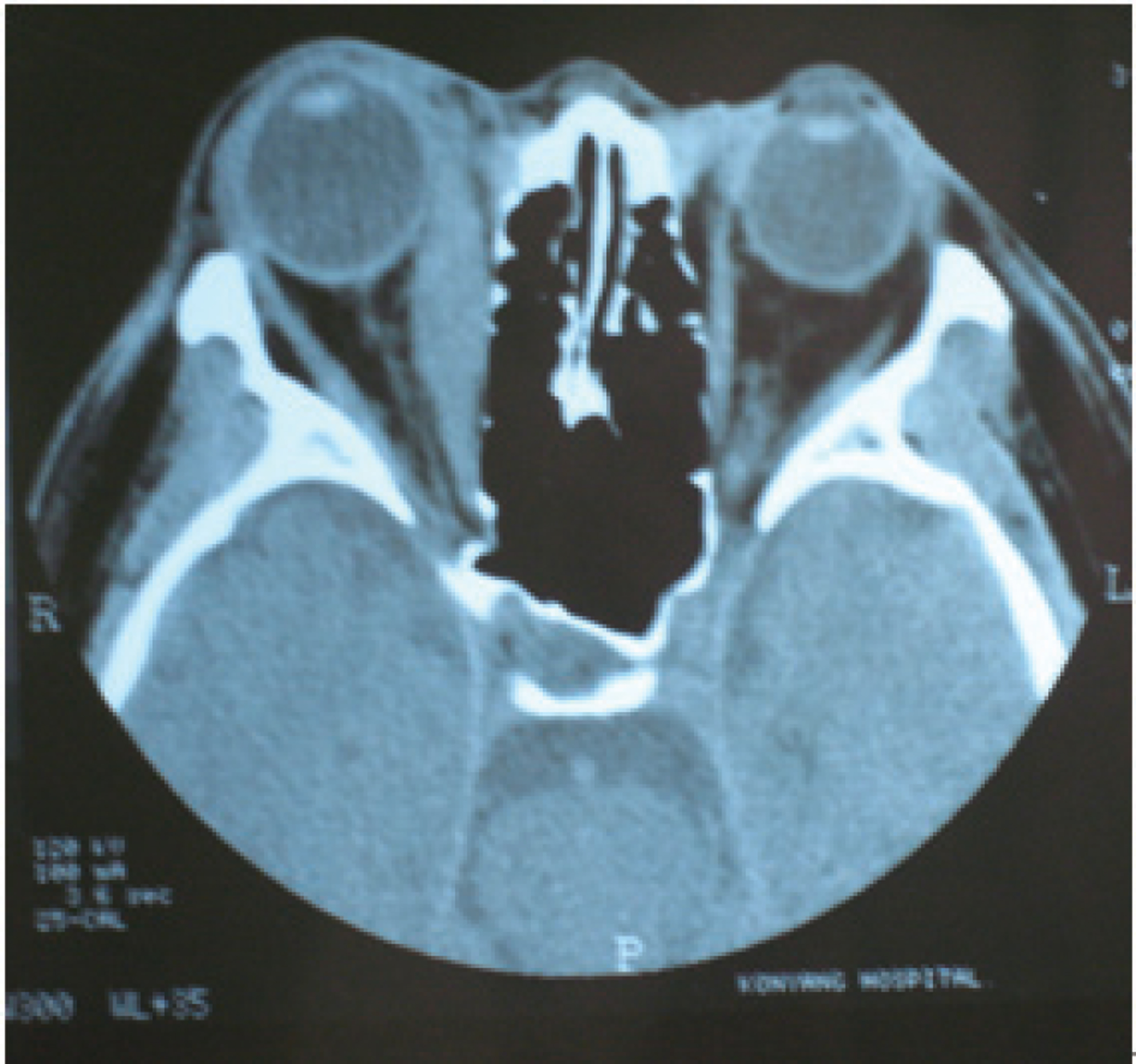
Figure 4. Myositic type, CT scan shows enlargement of the right medial rectus muscle with involvement of the tendon sheath..

Figure 5. Lacrimaltype, CT scan shows right lacrimal gland enlargement.
Reference
-
References
1. Günalp I, Gündüz K, Yazar Z. Idiopathic orbital inflammatory disease. Acta Ophthalmol Scand. 1996; 74:191–3.
Article2. Cervellini P, Volpin L, Curri D. . Sclerosing Orbital Pseudotumor. Ophthalmologica. 1986; 193:39–44.
Article3. Weber AL, Romo LV, Sabates NR. Pseudotumor of the orbit. Clinical, pathologic, and radiologic evaluation. Radiol Clin North Am. 1999; 37:151–68.4. Nugent RA, Rootman J, Robertson WK. . Acute orbital pseudotumors, classification and CT features. AJR Am J Roentgenol. 1981; 137:957–62.
Article5. Bencherif B, Zouaoui A, Chedid G. . Intracranial Extension of an Idiopathic Orbital Inflammatory Pseudotumor. AJNR Am J Neuroradiol. 1993; 14:181–4.6. Blodi FC, Gass JD. Inflammatory pseudotumor of the orbit. Br J Ophthalmol. 1968; 52:79–93.7. Blodi FC, Gass JD. Inflammatory pseudotumor of the orbit Trans Am Acad Ophthalmol Otolaryngol. 1967; 71:303–23.8. Scott I, Siatkowski RM. Idiopathic orbital myositis. Curr Opin Rheumatol. 1997; 9:504–12.
Article9. Char DH, Miller T. Orbital Pseudotumor, Fine-needle Aspiration Biopsy and Response to Therapy. Ophthalmology. 1993; 100:1702–10.10. Mombaerts I, Goldschmeding R, Schlingemann RO, Koornneef L. What is orbital Pseudotumor? Surv Ophthalmol. 1996; 41:66–78.11. Mannor GE, Rose GE, Moseley IF, Wright JE. Outcome of orbital myositis: clinical features associated with recurrence. Ophthalmology. 1997; 104:409–13.12. Mombaerts I, Koornneef L. Current status in the treatment of orbital myositis. Ophthalmology. 1997; 104:402–8.
Article13. Mombaerts I, Schlingemann RO, Goldschmeding R, Koornneff L. Are systemic corticosteroids useful in the management of orbital pseudotumor? Ophthalmology. 1996; 103:521–8.14. Moseley IF, Wright JE. Orbital pseudotumor. Clin Radiol. 1992; 45:67.15. Yuen SJ, Rubin PA. Idiopathic orbital inflammation: distribution, clinical features, and treatment outcome. Arch Ophthalmol. 2003; 121:491–9.16. Lee H, Kim SJ. Lee SY Classification and treatment efficacy of orbital psedotumor. J Korean Ophthalmol Soc. 2001; 42:1647–54.17. Henderson JW. Orbital Tumors, 2nd ed. New York: Decker/Thieme. Stratton. 1980; 512.18. Klein BR, Hedges TR, Dayal Y. . Orbital myositis and giant cell myocarditis. Neurology. 1989; 39:988–90.
Article19. Seidenberg KB, Leid ML. Orbital myositis with Lyme disease. Am J Ophthalmol. 1990; 109:13–6.
Article20. Volpe NJ, Shore JW. Orbital myositis associated with herpes zoster. Arch Ophthalmol. 1991; 109:471–2.
Article21. Orssaud C, Poisson M, Gaddeur D. Orbital myositis, recurrence of Whipple’s disease. J Fr Ophthalmol. 1992; 15:205–8.22. Maurer I, Zierz S. Recurrent orbital myosistis: report of a familial incidence. Arch Neurol. 1999; 56:1407–9.23. Lee JS, Yum BS, Choi CH, Kim HJ. Clinical study of the idiopatic orbital myositis. J Korean Ophthalmol Soc. 1999; 40:1109–15.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Features and Results of Steroid Therapy for Orbital Inflammatory Pseudotumor
- A Case of Orbital Pseudotumor
- Spontaneous Regression of Inflarmmatory Pseudotumor of the Liver by Conservative Therapy
- Fine Needle Aspiration Cytology of Inflammatory Pseudotumor of the Lung: Report of A Case Misdiagnosed as Adenocarcinoma
- Atypical Presentation of Orbital Pseudotumor with Visual Loss as an Initial Manifestation
