J Korean Ophthalmol Soc.
2007 Dec;48(12):1636-1642.
Cataract Formation after Penetrating Keratoplasty
- Affiliations
-
- 1Department of Ophthalmology, St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. eyedoc@catholic.ac.kr
Abstract
-
PURPOSE: To evaluate the risk factors for cataract formation and cataract extraction after penetrating keratoplasty to determine whether a combined surgery should be performed.
METHODS
Variables from 189 phakic eyes that underwent penetrating keratoplasty from April 1992 to November 2004 were analyzed for the possibility of cataract extraction after penetrating keratoplasty according to sex, age, diagnosis, accompanied glaucoma, preoperative vision and steroid use. The mean interval between penetrating keratoplasty and cataract extraction was also studied.
RESULTS
Cataract extraction was performed in 27 eyes (14.3%) and the mean interval between keratoplasty and cataract extraction was 24.5 months. Age was determined to be the most important independent risk factor for cataract extraction (p=0.0009) associated glaucoma also shown to be a risk factor (p=0.0011). Sex and corneal disease before keratoplasty were not shown to be risk factors. In the mean interval cataract extraction following penetrating keratoplasty, no statistically significant difference was found according to age, sex and diagnosis. Posterior subcapsular cataract was predominant (55.6%) and the mean visual acuity improved from 0.10 to 0.42.
CONCLUSIONS
The likelihood of cataract formation and cataract extraction subsequent to penetrating keratoplasty increased with age and associated glaucoma. The results from this study can help surgeons to determine whether combined surgery should be performed and help them to counsel patients on the risk of cataract formation.
MeSH Terms
Figure
-
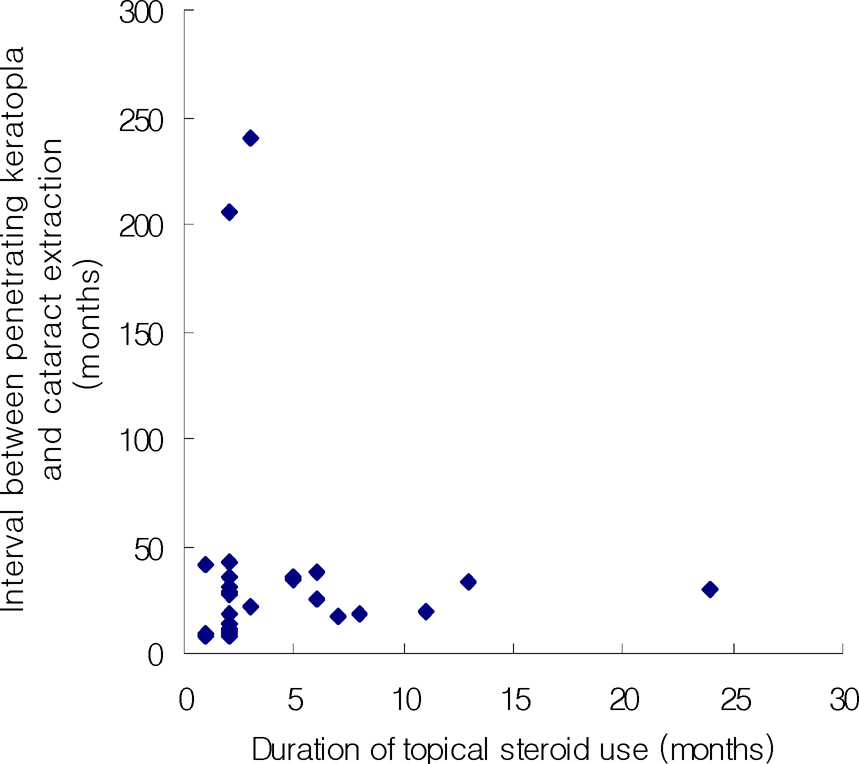
Figure 1. Relationship between topical steroid use and cataract formation
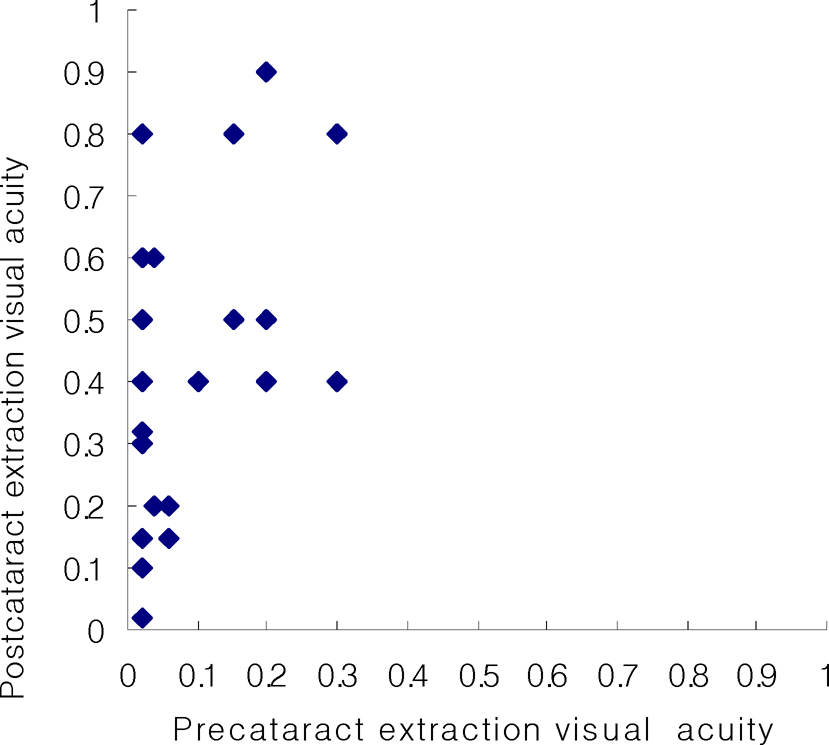
Figure 2. Relationship between precataract and postcataract extraction visual acuity
Reference
-
References
1. Katzin HM, Meltzer JF. Combined surgery for corneal transplantation and cataract extraction. Am J Ophthalmol. 1966; 62:556–60.
Article2. Casey TA. The combined operation of cataract and corneal graft. Trans Ophthalmol Soc U K. 1970; 89:659–68.3. Keates RH, Falkenstein S. Keratoplasty in keratoconus. Am J Ophthalmol. 1972; 74:442–4.
Article4. Kaufman HE. Combined keratoplasty and cataract extraction. Am J Ophthalmol. 1974; 77:824–9.
Article5. Capella JA, Kaufman HE, Polak FM. Prognosis of keratoplasty in phakic and aphakic patients and use of cryopreserved donor tissue. Trans Am Acad Ophthalmol Otolaryngol. 1972; 76:1275–85.6. Fine M. Therapeutic keratoplasty in fuchs’ dystrophy. Am J Ophthalmol. 1964; 57:371–8.
Article7. Stark WJ, Maumenee AE. Cataract extraction after successful penetrating keratoplasty. Am J Ophthalmol. 1973; 75:751–4.
Article8. Payant JA, Gordon LW, Vander Zwaag R, Wood TO. Cataract formation following corneal transplantation in eyes with Fuch's endothelial dystrophy. Cornea. 1990; 9:286–9.
Article9. Martin TP, Reed JW, Laugault C, et al. Cataract formation and cataract extraction after penetrating keratoplasty. Ophthalmology. 1994; 101:113–9.
Article10. Black RL, Oglesby RB, Von Sallmann L, Bunim JJ. Posterior subcapsular cataracts induced by corticosteroids in patients with rheumatoid arthritis. JAMA. 1960; 174:166–71.
Article11. Fournier C, Milot JA, Clermont M, O'Regan S. The concept of corticosteroid cataractogenic factor revisited. Can J Ophthalmol. 1990; 25:345–7.12. Shun-shin GA, Ratcliffe P, Bron AJ, et al. The lens after renal transplantation. Br J Ophthalmol. 1990; 74:267–71.
Article13. Adhikary HP, Sells RA, Basu PK. Ocular complications of systemic steroid after renal transplantation and their association with HLA. Br J Ophthalmol. 1982; 66:290–1.
Article14. Hilton AF, Harrison JD, Lamb AM, et al. Ocular complications in haemodialysis and renal transplant patients. Aust J Ophthalmol. 1982; 10:247–53.
Article15. Jobling AI, Augusteyn RC. What causes steroid cataract? A review of steroid-induced posterior subcapsular cataracts. Clin Exp Optom. 2002; 85:61–75.16. Spaeth GL, Von Sallman L. Corticosteroids and cataracts. Int Ophthalmol Clin. 1966; 6:915–28.
Article17. Sperduto RD, Hiller R. The prevalence of nuclear, cortical, and posterior subcapsular lens opacities in a general population sample. Ophthalmology. 1984; 91:815–8.18. Lin SY, Li MJ, Liang RC, Lee SM. Non-destructive analysis of the conformational changes in human lens lipid and protein structures of the immature cataracts associated with glaucoma. Spectrochim Acta A Mol Biomol Spectrosc. 1998; 54:1509–17.
Article19. Harding JJ, Harding RS, Egerton M. Risk factors for cataract in Oxfordshire diabetes, peripheral neuropathy, myopia, glaucoma and diarrhea. Acta Ophthalmol. 1989; 67:510–7.20. Leske MC, Wu SY, Nemesure B, Hennis A. Barbados Eye Studies Group. Risk factors for incident nuclear opacities. Ophthalmology. 2002; 109:1303–8.
Article21. Shaffer RN, Rosenthal G. Comparison of cataract incidence in normal and glaucomatous population. Am J Ophthalmol. 1970; 69:368–71.
Article22. Chandrasekaran S, Cumming RG, Rochitchina E, Mitchell P. Associations between elevated intraocular pressure and glaucoma, use of glaucoma medications, and 5-year incident cataract: the Blue Mountains Eye Study. Ophthalmology. 2006; 113:417–24.23. Ficker LA, Kirkness CM, Steel AD, et al. Intraocular surgery following penetrating keratoplasty. Eye. 1990; 4:693–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cataract Extraction after Penetrating Keratoplasty
- The Quadri: Combined Phototherapeutic Keratectomy, Penetrating Keratoplasty, Phacoemulsification and Posterior Chamber Lens Implantation
- Clinical Evaluation of the Glaucoma after Penetrating Keratoplasty
- Penetrating Keratoplasty for Bullous Keratopathy following Cataract Extraction
- Combined Keratoplasty and Cataract Surgery
