Injury Severity and Patterns of Accompanying Injury in Spinal Fracture
- Affiliations
-
- 1Department of Orthopedic Surgery, Gwangju Veterans Hospital, Gwangju, Korea.
- 2Department of Orthopedic Surgery, Chonbuk National University Medical School, Research Institute of Clinical Medicine, Chonbuk National University Hospital, Jeonju, Korea. osdr2815@naver.com
Abstract
- PURPOSE
To examine the relationship between injury severity and patterns of associated injury in spinal fracture.
MATERIALS AND METHODS
From March 2004 to March 2010, a retrospective study was conducted on 291 patients who had undergone surgeries due to spinal fractures. Spinal fractures were categorized as upper cervical, lower cervical, thoracic, thoracolumbar, and lumbar region, and the severity of fracture was measured using the Abbreviated Injury Scale and Injury Severity Score (ISS). We evaluated the correlation between the fracture site and the incidence and injury severity of the associated injury, and compared the neurologic damage according to the presence/absence of the associated injury.
RESULTS
Spinal fracture occurred in the thoracic (43.5%) and lower cervical (30.0%) levels, and associated injury developed in 134 patients (47%). The area of associated injury was in the extremity (41.2%), thorax (25.5%), head, neck, and face (21.9%). Lower cervical fracture (34.5%) had a lower prevalence than thoracic (81%) and lumbar fracture (61%). The average ISS of the associated injury was 17.14 for the thoracic fracture, 12.30 for the lower cervical fracture, 8.7 for the thoracolumbar fracture and 5.69 for the lumbar fracture. Neurologic damage was highly frequent in the lower cervical fracture and included 54 patients (62.1%) and was less frequent in the upper cervical fracture, which included 7 patients (17.9%) (p=0.032).
CONCLUSION
Although the associated injury was less frequent in the lower cervical spine among the spinal fractures that underwent surgical treatment, there was a high risk of neurologic damage in the case of associated injury; therefore, there is a need to pay special attention to patients that suffer damage in this area. In addition, since the degree of the associated injury in the thoracic and lower cervical fracture is significant, an appropriate management strategy for the associated injury must be considered.
Keyword
MeSH Terms
Figure
-
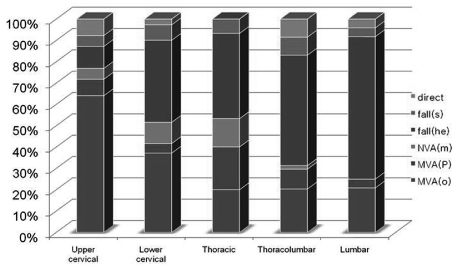
Fig. 1 The histogram demonstrates the relationship between the location of the associated injury and the injury mechanism. Direct trauma and others, Fall (s): fall from standing, Fall (he): fall from height, MVA (m): motor vehicle accident, motorcyclist, MVA (p): motor vehicle accident, pedestrian, MVA (o): motor vehicle accident, occupant.

Fig. 2 The histogram demonstrates the incidence of associated injury according to the location of the vertebral fracture.
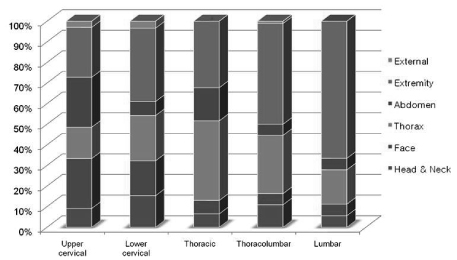
Fig. 3 The histogram demonstrates the distribution and frequency ofassociated injuries according to the location of the vertebral fracture.
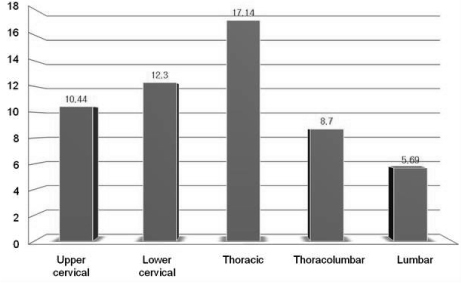
Fig. 4 The histogram demonstrates the Injury Severity Score of the associated injuries according to the location of the vertebral fracture.

Fig. 5 The histogram demonstrates the incidence of neurologic deficit according to the location of the vertebral fracture.
Reference
-
1. Baker SP, O'Neill B, Haddon W Jr, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974. 14:187–196.
Article2. Bensch FV, Kiuru MJ, Koivikko MP, Koskinen SK. Spine fractures in falling accidents: analysis of multidetector CT findings. Eur Radiol. 2004. 14:618–624.
Article3. Chawda MN, Hildebrand F, Pape HC, Giannoudis PV. Predicting outcome after multiple trauma: which scoring system? Injury. 2004. 35:347–358.
Article4. Choi ES, Kim YM, Kim DS, et al. Differences of fracture types and associated injuries in thoracolumbar fractures caused by fall from height and by in-Car accident. J Korean Fract Soc. 2005. 18:176–180.
Article5. Civil ID, Schwab CW. The Abbreviated Injury Scale, 1985 revision: a condensed chart for clinical use. J Trauma. 1988. 28:87–90.6. Dai LY, Yao WF, Cui YM, Zhou Q. Thoracolumbar fractures in patients with multiple injuries: diagnosis and treatment-a review of 147 cases. J Trauma. 2004. 56:348–355.7. Hu R, Mustard CA, Burns C. Epidemiology of incident spinal fracture in a complete population. Spine (Phila Pa 1976). 1996. 21:492–499.
Article8. Levin AM, Edwards CC. Camins MB, O'Leary PF, editors. Lumbar spine trauma. The lumbar spine. 1987. New York: Raven Press;183–212.
Article9. Saboe LA, Reid DC, Davis LA, Warren SA, Grace MG. Spine trauma and associated injuries. J Trauma. 1991. 31:43–48.10. Shin BJ, Kim BW, Kim YI, Rah SK. Differences of fracture patterns by the level of the thoracolumbar and lumbar burst fractures. J Korean Soc Spine Surg. 1998. 5:47–52.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Neurologic Injury and Recovery Patterns in the Spinal Fractures by Denis Classification
- Neurologic Recovery According to the Spinal Fracture Patterns by Denis Classification
- Dysesthetic Pain Syndrome in Spinal Cord Injury Patients
- Statistical observation of the spine injury
- An Analysis of Cranio-spinal Fracture in Case of Free-falling Trauma
