Analysis of Effect of Inferior Oblique Myectomy in Patients With Inferior Oblique Overaction
- Affiliations
-
- 1Department of Ophthalmology, Hallym University College of Medicine, Seoul, Korea. eyechoi@dreamwiz.com
- KMID: 2214140
- DOI: http://doi.org/10.3341/jkos.2011.52.1.67
Abstract
- PURPOSE
To investigate the effect of inferior oblique (IO) myectomy by analyzing the correlation of the amount of inferior oblique overaction (IOOA), hypertropia and excyclotorsion before, between, and after IO myectomy in patients with various degrees of IOOA.
METHODS
A total of 86 eyes from 59 patients with IOOA who underwent IO myectomy were enrolled in the present study. The correlation analysis was performed for the amount of IOOA, hypertropia and excyclotorsion before and after surgery, according to the preoperative amount of IOOA, hypertropia, and excyclotorsion.
RESULTS
The IOOA decreased from +2.5 +/- 0.6 before surgery to -0.01 +/- 0.25 (p < 0.05) after surgery. The vertical deviation was 5.7 +/- 6.3 prism diopter (PD) and 2.3 +/- 5.2 PD (p < 0.05) postoperatively. The amount of cyclodeviation was 15.3 +/- 7.6degrees before surgery and 6.6 +/- 5.7degrees (p < 0.05) after surgery. The amount of surgical correction for IOOA and the hypertropia was significantly correlated with preoperative deviation (p < 0.05, p < 0.05). The amount of excyclotorsion before and after surgery was also positively correlated but was not statistically significant (p = 0.05).
CONCLUSIONS
IO myectomy can correct any degree of IOOA, hypertropia, and related excyclotorsion.
MeSH Terms
Figure
-
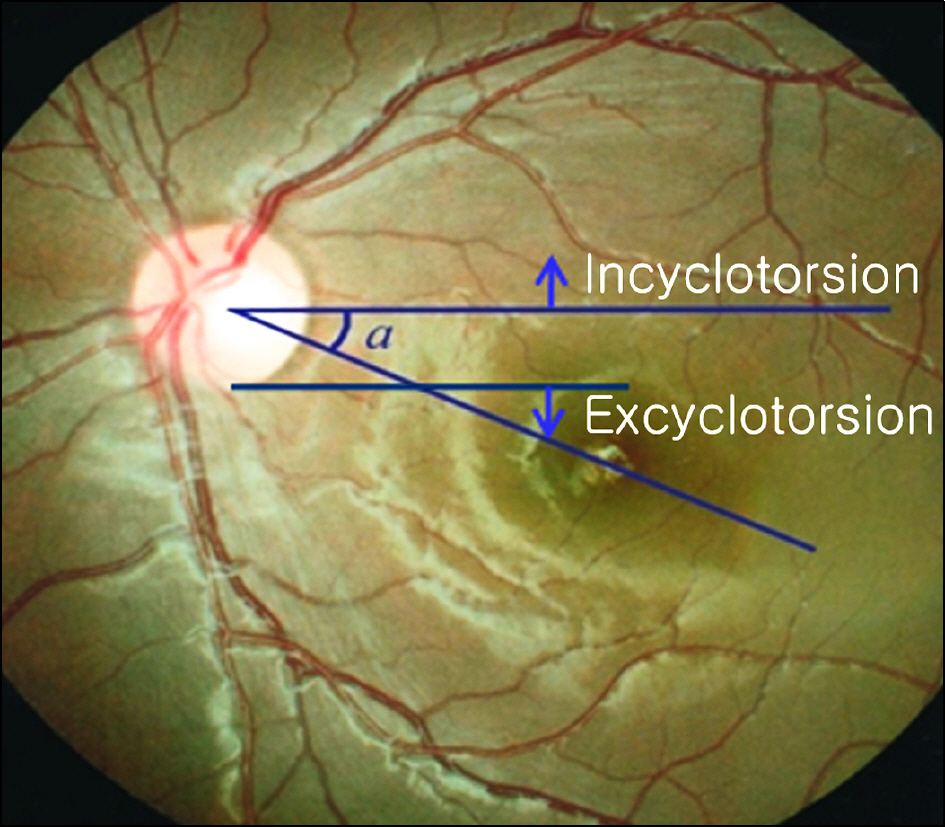
Figure 1. Measurement of cyclotorsion on fundus photograph. The angle (α) between horizontal line and imaginary line across the center of the macula and optic nerve head was measured.
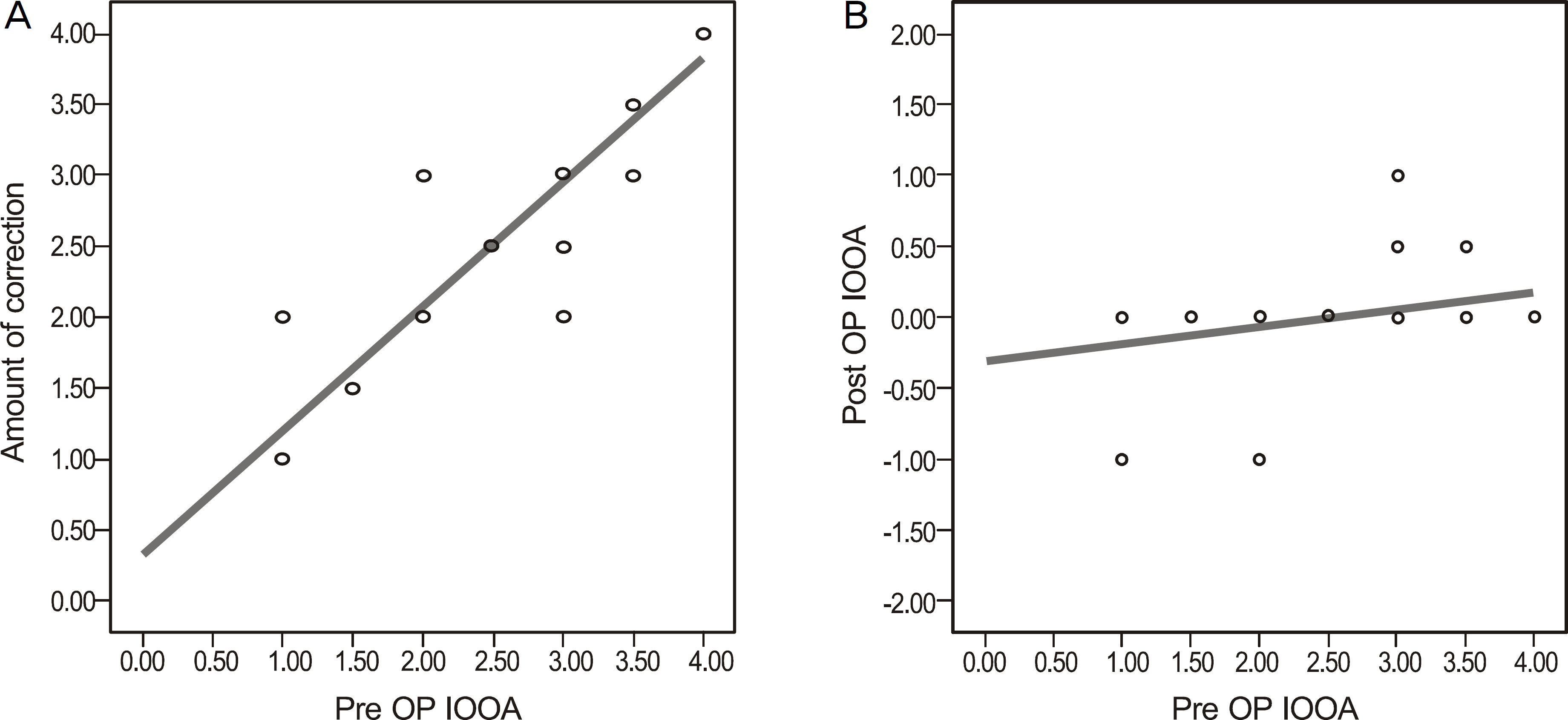
Figure 2. The preexisting IOOA (inferior oblique muscle overaction) positively correlated with the amount of correction (Pearson's correlation coefficiency, r = 0.927, R2 = 0.86, p < 0.05) (A) and with the postoperative residual IOOA significantly (r = 0.318, R2 = 0.101, p < 0.05) (B).
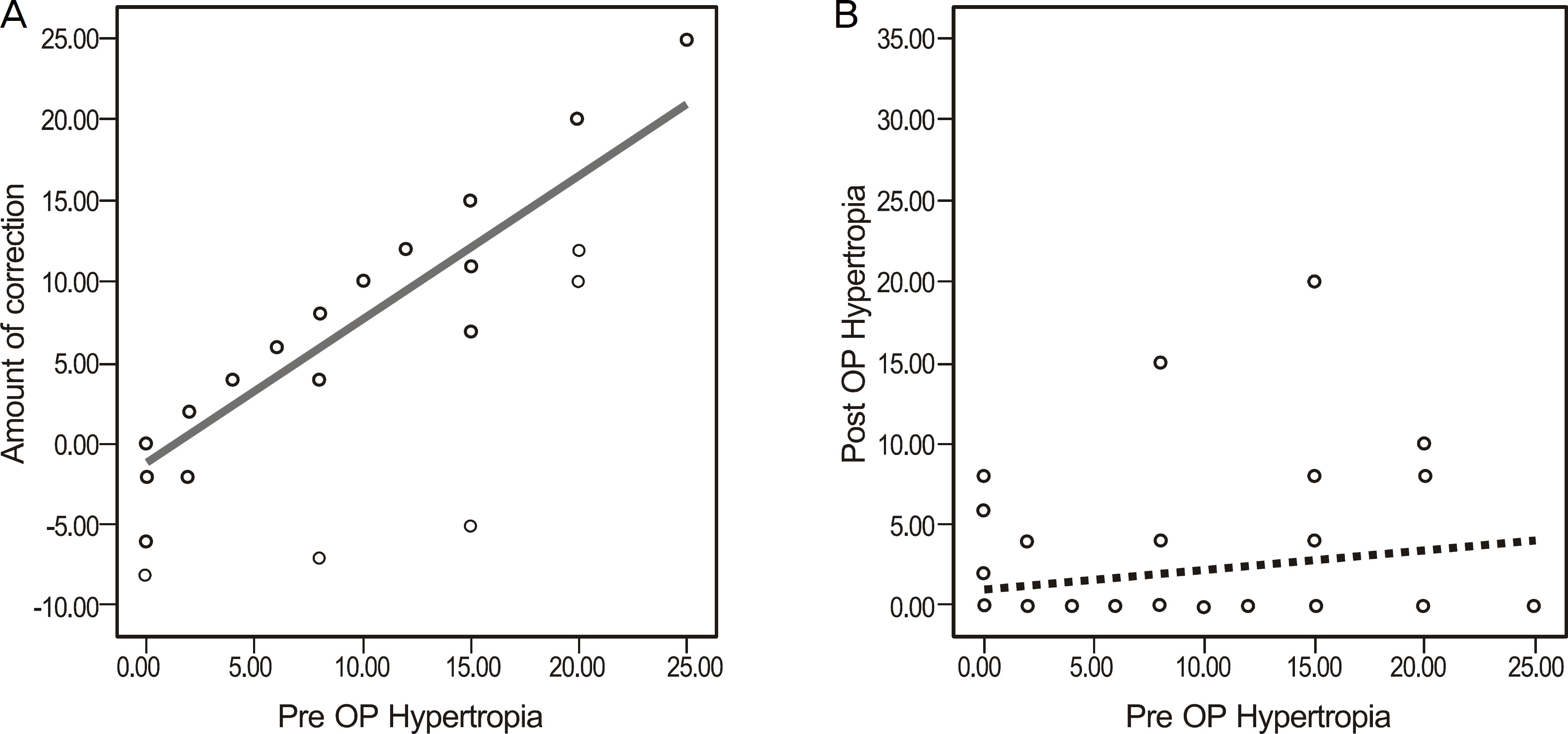
Figure 3. The preexisting hypertropia in primary gaze positively correlates with the amount of correction (Pearson's correlation coefficiency, r = 0.837, R2 = 0.701, p < 0.05) (A) but not with the postoperative residual hypertropia (r = 0.202, R2 = 0.041, p = 0.092) (B).
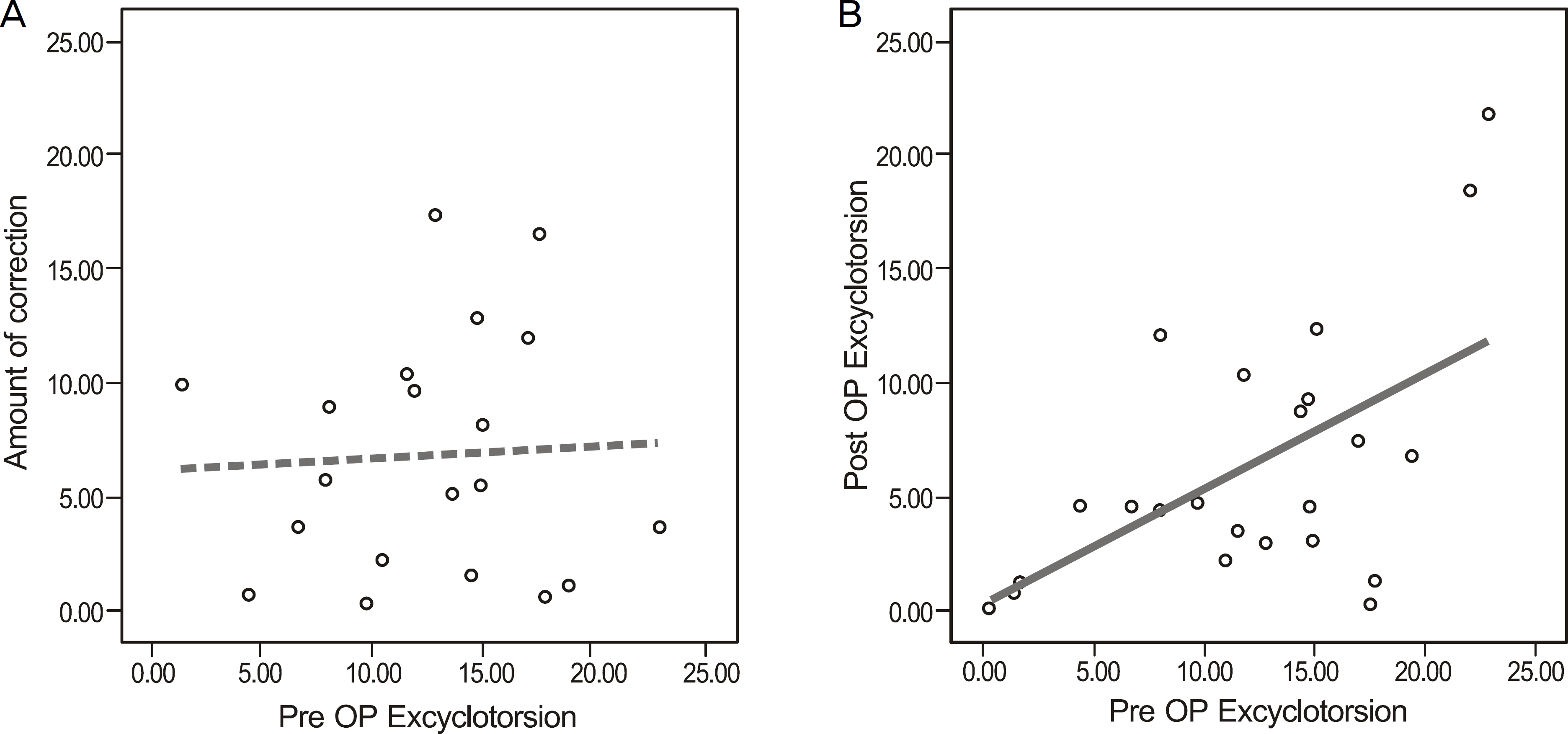
Figure 4. The preexisting excyclotorsion dosen't correlate with the amount of correction significantly (Pearson's correlation coefficiency, r = 0.051, R2 = 0.003, p = 0.832) (A). But the preexisting excyclotorsion positively correlates with the postoperative residual excyclotorsion (r = 0.572, R2 = 0.328, p < 0.05) (B).
Cited by 1 articles
-
Changes in Ocular Excyclotorsion According to Graded Inferior Oblique Recession
Donghun Lee, Won Jae Kim, Myung Mi Kim
J Korean Ophthalmol Soc. 2016;57(8):1268-1273. doi: 10.3341/jkos.2016.57.8.1268.
Reference
-
References
1. Ghazawy S, Reddy AR, Kipioti A, et al. Myectomy versus anterior transposition for inferior oblique overaction. J AAPOS. 2007; 11:601–5.
Article2. Plager DA. Oblique muscle dysfunction. Plager DA, editor. Strabismus Surgery Basic and Advanced Strategies. New York: Oxford University Press;2004. chap. 3.3. Ziffer AJ, Isenberg SJ, Elliott RL, Apt L. The effect of anterior transposition of the inferior oblique muscle. Am J Ophthalmol. 1993; 116:224–7.
Article4. Cho YA, Kim JH, Kim S. Antielevation syndrome after unilateral anteriorization of the inferior oblique muscle. Korean J Ophthalmol. 2006; 20:118–23.
Article5. Kushner BJ. Restriction of elevation in abduction after inferior oblique anteriorization. J AAPOS. 1997; 1:55–62.
Article6. Mims JL 3rd, Wood RC. Antielevation syndrome after bilateral anterior transposition of the inferior oblique muscles: incidence and prevention J AAPOS. 1999; 3:3336.7. Shipman T, Burke J. Unilateral inferior oblique muscle myectomy and recession in the treatment of inferior oblique muscle overaction: a longitudinal study. Eye. 2003; 17:1013–8.
Article8. Min BM, Park JH, Kim SY, Lee SB. Comparison of inferior oblique muscle weakening by anterior transposition or myectomy: a prospective study of 20 cases. Br J Ophthalmol. 1999; 83:206–8.9. Chang BL, Chang MH, Yang SW. Inferior oblique overaction. J Korean Ophthalmol Soc. 1988; 29:1065–9.
Article10. Rho IH, Choi MY. The effect of myectomy on the grading of overaction of the inferior oblique muscle. J Korean Ophthalmol Soc. 2006; 47:437–42.11. Mellott ML, Scott WE, Ganser GL, et al. Marginal myotomy of the minimally overacting inferior oblique muscle in asymmetric bilateral superior oblique palsies. J AAPOS. 2002; 6:216–20.
Article12. Parks MM. The weakening surgical procedures for eliminating overaction of the inferior oblique muscle. Am J Ophthalmol. 1972; 73:107–22.
Article13. Elliott RL, Nankin SJ. Anterior transposition of the inferior oblique. J Pediatr Ophthalmol Strabismus. 1981; 18:35–8.
Article14. Rubinstein K, Dixon J. Myectomy of the inferior oblique; report on 100 cases. Br J Ophthalmol. 1959; 43:21–8.
Article15. Song BY, Park SW, Park YG. The surgical effect of inferior oblique anteriorization. J Korean Ophthalmol Soc. 2004; 45:995–1000.16. Guemes A, Wright KW. Effect of graded anterior transposition of the inferior oblique muscle on versions and vertical deviation in primary position. J AAPOS. 1998; 2:201–6.
Article17. Jones TW Jr, Lee DA, Dyer JA. Inferior oblique surgery. aberrations at the Mayo Clinic from 1960 to 1981. Arch Ophthalmol. 1984; 102:714–6.18. Shin YJ, Lee TS. Effect of myectomy on overacting inferior oblique muscle. J Korean Ophthalmol Soc. 1984; 25:347–51.19. Stuart JA. Myectomy of the inferior oblique muscle. Am J Ophthalmol. 1964; 57:118–21.
Article20. Dunlap EA. Inferior oblique weakening. Recession, myotomy, myectomy, or disinsertion? Ann Ophthalmol. 1972; 4:905–12.21. Davis G, McNeer KW, Spencer RF. Myectomy of the inferior oblique muscle. Arch Ophthalmol. 1986; 104:855–8.
Article22. Rosenbaum AL, Santiago AP. Clinical strabismus management. Philadelphia: W.B. Saunders Company;1999. p. 17.23. Bixenman WW, von Noorden GK. Apparent foveal displacement in normal subjects and in cyclotropia. Ophthalmology. 1982; 89:58–62.
Article24. Lee DH, Lee SJ, Park SH. Ocular torsion in normal Korean population. J Korean Ophthalmol Soc. 2004; 45:797–802.25. Park SW. The torsional status of normal Koreans. J Korean Ophthalmol Soc. 2004; 45:1906–11.26. Parks MM. Causes of the adhesive syndrome. Symposium on strabismus. Transactions of the New Orleans Academy of aberrationsogy. St. Louis: The C.V. Mosby Company;1978. p. 269–79.27. Cho YA, Kim SH. Surgical outcomes of intermittent exotropia associated with concomitant hypertropia including simulated superior oblique palsy after horizontal muscles surgery only. Eye. 2007; 21:1489–92.
Article28. Von Noorden GK. Binocular vision and ocular motility. 6th ed.St. Louis: Mosby;2002. p. 396–413.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison between Myectomy and Anterior Transposition on Inferior Oblique Overaction
- Secondary Superior Oblique Overaction after Inferior Oblique Muscle Myectomy in a Patient Misdiagnosed with Inferior Oblique Muscle Overaction
- The Effect of Myectomy on the Grading of Overaction of the Inferior Oblique Muscle
- The Effect of Anteriorization of The Inferior Oblique Muscle in +3 or +4 Inferior Oblique Overaction
- Inferior Oblique Overaction
