Learning Curve for the Thoracoscopic Correction of Spinal Deformities
- Affiliations
-
- 1Department of Orthopaedic Surgery, Yonsei University, Seoul, Korea. haksunkim@yumc.yonsei.ac.kr
- 2Department of Orthopaedic Surgery, National Health Insurance Corporation Ilsan Hospital.
- 3Department of Orthopaedic Surgery, Pochon CHA University.
- KMID: 2209695
- DOI: http://doi.org/10.4184/jkss.2003.10.3.261
Abstract
- STUDY DESIGN: Twenty-six consecutive cases were prospectively studied by chart review and radiography.
OBJECTIVES
The aim of this study was to find the learning curve of spinal thoracoscopy in spinal deformity surgery. SUMMARY OF LITERATURE REVIEW : Although the efficacy and learning curve of thoracoscopic deformity spinal surgery are well documented in many countries, there is no report in Korea.
METHODS
Twenty-six consecutive patients who were underwent VATS were studied. Idiopathic scoliosis was diagnosed in 23 patients (King type II in 15, type III in 5, type IV in 3), neuromuscular scoliosis in 2 and kyphotic deformity in one. In 14 cases of idiopathic scoliosis VATS for anterior release, bonegraft and instrumentation were performed. In the remaining 12 cases of anterior release, bone graft by VATS was done without instrumentation.
RESULTS
The average number of discs excised was 5.2+/-0.97. The average time of surgery for the 14 cases was 7.3+/-1.3 hours, which represented 1.37+/-0.25 hours per disc. Excluding the time of instrumentation in the 26 cases, the average time for anterior release and bone grafting was 3.87+/-0.87 hours, which represented 0.76+/-0.18 hours per disc. The average operation time diminished as the series continued. Average blood loss was 748.9+/-254 mL, which represented 152.6+/-65.6 mL per disc. The Cobb's angle was corrected by 62% on average. Complications were found in 11 cases: screw cap breakage in 3, atelectasis in 4, and intercostal nerve injury in 4. There was no serious complication.
CONCLUSIONS
VAST for spinal deformity is a safe and effective alternative to thoracotomy, however, the learning curve for this procedure is quite difficult.
Keyword
MeSH Terms
Figure
-
Fig. 1. The portals of the thoracoscopic spinal deformity surgery should be located in the axillary line.

Fig. 2. Harmonic Scarlpel is very useful and convenient devise for bleeding control.

Fig. 3. The K-wire can be used as the marker in the intra-operative fluorescopy exam.

Fig. 4. Two instruments were invented for rod de-rotation and screw wing cutting under the thoracoscopic guide.

Fig. 5. The screw cap was broken during the wing cutting.
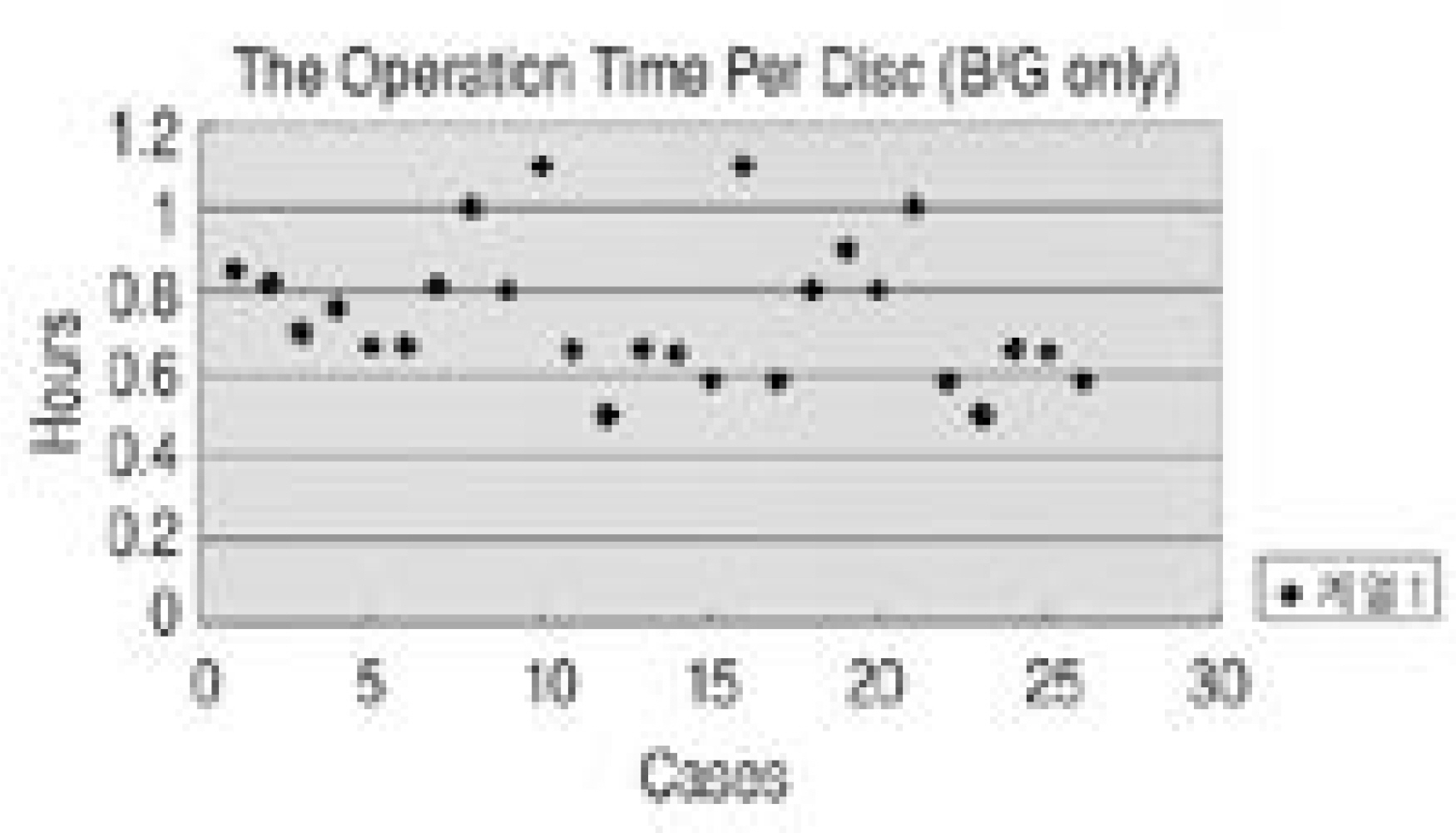
Fig. 6. The operating time per disc by case number in total case (n=26).

Fig. 7. Total operation time in instrumented cases (n=14).

Fig. 8. Operating time per disc by case number in instrumented case (n=14).
Cited by 1 articles
-
Sagittal Plane Analysis of Adolescent Idiopathic Scoliosis after VATS (Video-Assisted Thoracoscopic Surgery) Anterior Instrumentations
Hak-Sun Kim, Chong-Suh Lee, Byoung-Ho Jeon, Jin-Oh Park
Yonsei Med J. 2007;48(1):90-96. doi: 10.3349/ymj.2007.48.1.90.
Reference
-
1). Jacobeaus J. The cautrization of adhesion in pneumotho -rax treatment of tuberculosis. Surg Gynecol Obstract. 1921; 32:493–500.2). Hazelrigg SR, Landreneau RJ, Boley TM, et al. T he effect of muscle-sparing versus standard posterolateral thoracotomy on pulmonary function, muscle strength, and postoperative pain. J Thorac Cardiovasc Surg. 1991; 101:394–400.3). Landreneau RJ, Hazelrigg SR, Mack MJ, et al. Postoperative pain-related morbidity: video-assisted thoracic surgery versus thoracotomy. Ann Thorac Surg. 1993; 56:1285–1289.
Article4). Newton PO, Wenger DR, Mubarak SJ and Meyer RS. Anterior release and fusion in pediatric spinal deformity. A comparison of early outcome and cost of thoracoscopic and open thoracotomy approaches. Spine. 1998; 22:1398–1406.5). Huntington CF, Murrell WD, Betz RR, Cole BA, Clements DH 3rd and Balsara RK. Comparison of thoracoscopic and open thoracic discectomy in a live ovine model for anterior spinal fusion. Spine. 1998; 23:1699–1702.
Article6). Newton PO, Cardelia JM, Farnsworth CL, Baker KJ and Bronson DG. A biomechanical comparison of open and thoracoscopic anterior spinal release in a goat model. Spine. 1998; 23:530–535.
Article7). Wall EJ, Bylski-Austrow DI, Shelton FS, Crawford AH, Kolata RJ and Baum DS. Endoscopic discectomy increases thoracic spine flexibility as effectively as open discectomy: A mechanical study in a porcine model. Spine. 1998; 23:9–15.8). McAfee PC, Regan JR, Zdeblick T, et al. The incidence of complications in endoscopic anterior thoracolumbar spinal reconstructive surgery: A prospective multicenter study comprising the first 100 consecutive cases. Spine. 1995; 20:1624–1632.9). Kaiser LR and Bavaria JE. Complications of thoracoscopy. Ann Thorac Surg. 1993; 56:796–798.10). Picetti GD 3rd, Pang D and Bueff HU. Thoracosco pic techniques for the treatment of scoliosis: early results in procedure development. Neurosurgery. 2002; 51:978–984.11). Early SD, Newton PO, White KK, Wenger DR and Mubarak SJ. The feasibility of anterior thoracoscopic spine surgery in children under 30 kilograms. Spine. 2000; 27:2368–2373.
Article12). Huang EY, Acosta JM, Gardocki RJ, et al. Thor aco -scopic anterior spinal release and fusion: evolution of a faster, improved approach. J Pediatr Surg. 2002; 37:1732–1735.13). Newton PO, Shea KG and Granlund KF. Defining the pediatric spinal thoracoscopy learning curve: sixty-five consecutive cases. Spine. 2000; 25:1028–1235.14). Neilipovitz DT, Murto K, Hall L, Barrowman NJ and Splinter WM. A randomized trial of tranexamic acid to reduce blood transfusion for scoliosis surgery. Anesth Analg. 2001; 93:82–87.
Article15). Sucato DJ, Welch RD, Pierce B, Zhang H and Haideri N Bronson D. Thoracoscopic discectomy and fusion in an animal model: safe and effective when segmental blood vessels are spared. Spine. 2002; 27:880–886.16). Huang TJ and Hsu RW. Chylothorax after video-assist -ed thoracoscopic release for rigid scoliosis. Orthopedics. 2001; 24:789–790.17). Sucato DJ and Girgis M. Bilateral pneumothoraces, pneumomediastinum, pneumoperitoneum, pneu -moretroperitoneum, and subcutaneous emphysema following intubation with a double-lumen endotracheal tube for thoracoscopic anterior spinal release and fusion in a patient with idiopathic scoliosis. Spinal Disord Tech. 2002; 15:133–138.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Learning Curve for Thoracoscopic Repair of Congenital Diaphragmatic Hernia Using Cumulative Sum Analysis
- Clinical and Radiological Analysis of Thoracoscopic Spinal Surgery in Thoracolumbar Burst Fracture
- Clinical Analysis of Video-assisted Thoracoscopic Spinal Surgery in the Thoracic or Thoracolumbar Spinal Pathologies
- Deep Learning in MR Motion Correction:a Brief Review and a New Motion Simulation Tool (view2Dmotion)
- The Correction of Severe Spinal Kyphotic Deformities with Halo-pelvic Apparatus
