J Korean Soc Radiol.
2010 Mar;62(3):219-225. 10.3348/jksr.2010.62.3.219.
Self-Expandable Metallic Stent for the Palliative Treatment of Obstructing Left-Sided Colorectal Cancer under Fluoroscopic Guidance: A Comparison of the Clinical Results according to Stent Diameter
- Affiliations
-
- 1Department of Radiology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Korea. summerson@paran.com
- 2Department of Radiology, Kangwon National University College of Medicine, Korea.
- KMID: 2208916
- DOI: http://doi.org/10.3348/jksr.2010.62.3.219
Abstract
-
PURPOSE: To evaluate the feasibility, effectiveness, and safety of self-expandable metallic stent for the palliative treatment of obstructing left-sided colorectal cancer under fluoroscopic guidance, and to compare results according to the stent diameter.
MATERIALS AND METHODS
Under fluoroscopic guidance, 31 self-expandable metallic stents were placed into 25 patients for palliative purposes. The rates of technical success, clinical success, complications associated with stent insertion, patient survival, and primary stent patency were evaluated. The results were also compared between two groups: 13 patients using stents with a diameter of 22 mm and 12 patients using stents with a diameter of 26 mm.
RESULTS
The technical and clinical success rates were 93.5 and 90.3%, respectively. The complications included severe abdominal pain (6.5%), minor rectal bleeding (9.7%), stent migration (9.7%), and tumor ingrowth or overgrowth (9.7%). No statistical differences in technical were detected between the two groups for the clinical success rate and complication rates. The mean survival time was 5.5 +/- 1.4 months. The primary stent patency rates were 91.3% at 5 months, 85.2% at 10 months, and 77.4% at 15 months. The mean period of stent patency was 12.4 +/- 2.6 months. The mean period of primary stent patency was 16.4 +/- 2.6 months in the 26 mm stent group, and significantly higher than 5.4 +/- 1.4 months in the 22 mm stent group (p=0.031).
CONCLUSION
A self-expandable metallic stent under fluoroscopic guidance, for the palliative treatment of obstructing left-sided colorectal cancer, was feasible and effective, and yielded good clinical results. The period of primary stent patency of the 26 mm stent group was longer than the 22 mm stent group, and the complication rate was not significantly different between the two stent groups.
MeSH Terms
Figure
-
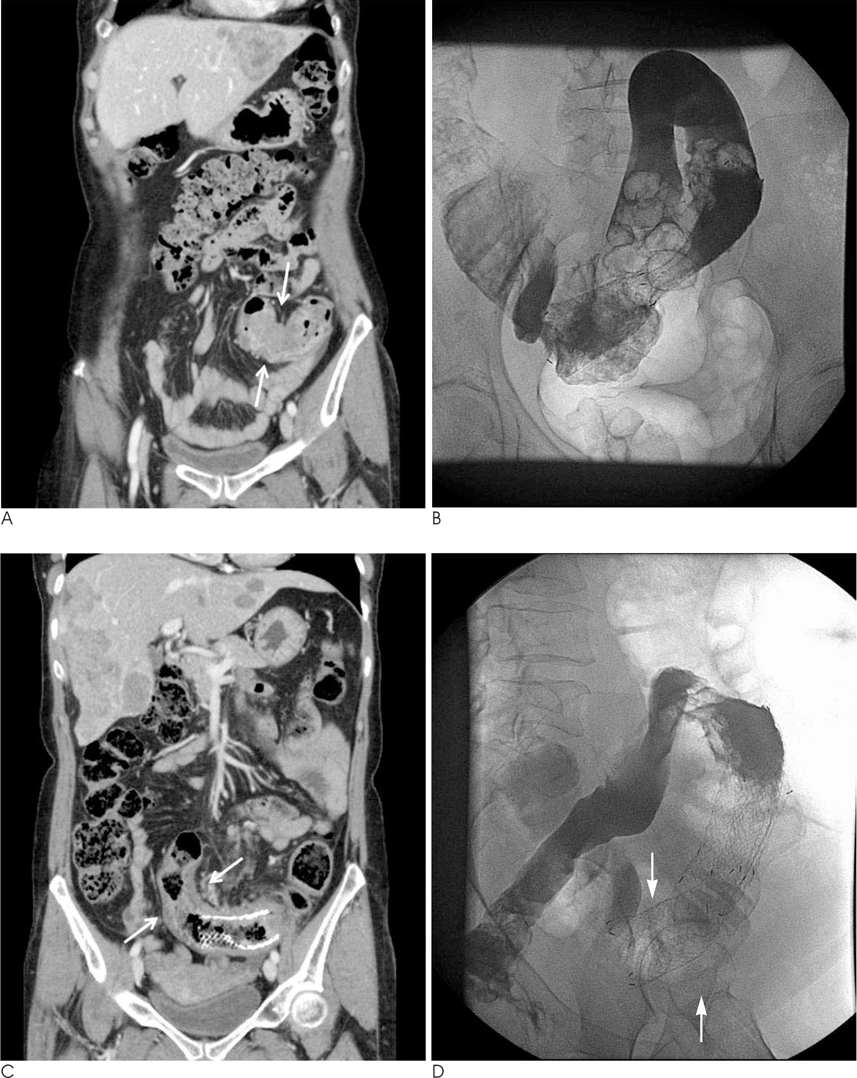
Fig. 1 59-year-old women. Coronal reformatted CT image (A) show asymmetric wall thickening at distal portion of descending colon (arrows). Multiple hepatic metastasis also noted. Endoscopic biopsy proved adenocarcinoma. 26 mm × 10 cm, covered stent inserted successfully (B). 3 months later, coronal reformatted CT image (C) show increased tumor extent to proximal portion of stent (arrows). Additional 26 mm × 12 cm, noncovered stent inserted successfully (arrows) (D).
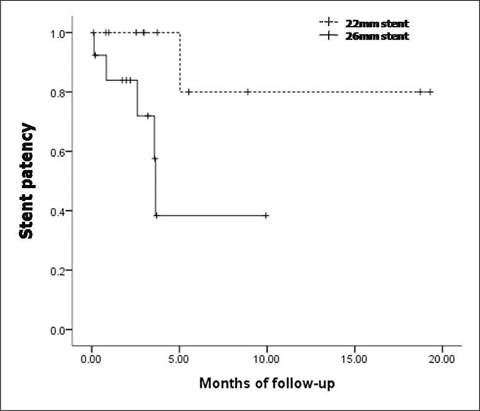
Fig. 2 Graph shows cumulative primary patency rate of 22 mm stent group and 26 mm stent group.
Reference
-
1. Umpleby HC, Williamson RC. Survival in acute obstructing colorectal carcinoma. Dis Colon Rectum. 1984; 27:299–304.2. Yu BM. Surgical treatment of acute intestinal obstruction caused by large bowel carcinoma. Zhonghua Wai Ke Za Zhi. 1989; 27:285–286.3. Bokey EL, Chapuis PH, Fung C, Hughes WJ, Koorey SG, Brewer D, et al. Postoperative morbidity and mortality following resection of the colon and rectum for cancer. Dis Colon Rectum. 1995; 38:480–487.4. Fielding LP, Phillips RK, Hittinger R. Factors influencing mortality after curative resection for large bowel cancer in elderly patients. Lancet. 1989; 1:595–597.5. Law WL, Choi HK, Chu KW. Comparison of stenting with emergency surgery as palliative treatment for obstructing primary leftsided colorectal cancer. Br J Surg. 2003; 90:1429–1433.6. Leitman IM, Sullivan JD, Brams D, DeCosse JJ. Multivariate analysis of morbidity and mortality from the initial surgical management of obstructing carcinoma of the colon. Surg Gynecol Obstet. 1992; 174:513–518.7. Mulcahy HE, Skelly MM, Husain A, O'Donoghue DP. Long-term outcome following curative surgery for malignant large bowel obstruction. Br J Surg. 1996; 83:46–50.8. Tejero E, Fernandez-Lobato R, Mainar A, Montes C, Pinto I, Fernandez L, et al. Initial results of a new procedure for treatment of malignant obstruction of the left colon. Dis Colon Rectum. 1997; 40:432–436.9. Law WL, Chu KW, Ho JW, Tung HM, Law SY, Chu KM. Self-expanding metallic stent in the treatment of colonic obstruction caused by advanced malignancies. Dis Colon Rectum. 2000; 43:1522–1527.10. Liberman H, Adams DR, Blatchford GJ, Ternent CA, Christensen MA, Thorson AG. Clinical use of the self-expanding metallic stent in the management of colorectal cancer. Am J Surg. 2000; 180:407–412.11. Turegano-Fuentes F, Echenagusia-Belda A, Simo-Muerza G, Camunez F, Munoz-Jimenez F, Del Valle, et al. Transanal self-expanding metal stents as an alternative to palliative colostomy in selected patients with malignant obstruction of the left colon. Br J Surg. 1998; 85:232–235.12. Mainar A, De Gregorio, Tejero E, Tobio R, Alfonso E, Pinto I, et al. Acute colorectal obstruction: treatment with self-expandable metallic stents before scheduled surgery--results of a multicenter study. Radiology. 1999; 210:65–69.13. Binkert CA, Ledermann H, Jost R, Saurenmann P, Decurtins M, Zollikofer CL. Acute colonic obstruction: clinical aspects and costeffectiveness of preoperative and palliative treatment with self-expanding metallic stents--a preliminary report. Radiology. 1998; 206:199–204.14. Saida Y, Sumiyama Y, Nagao J, Takase M. Stent endoprosthesis for obstructing colorectal cancers. Dis Colon Rectum. 1996; 39:552–555.15. Camunez F, Echenagusia A, Simo G, Turegano F, Vazquez J, Barreiro-Meiro I. Malignant colorectal obstruction treated by means of self-expanding metallic stents: effectiveness before surgery and in palliation. Radiology. 2000; 216:492–497.16. Alcantara M, Serra X, Bombardo J, Falco J, Perandreu J, Ayguavives I, et al. Colorectal stenting as an effective therapy for preoperative and palliative treatment of large bowel obstruction: 9 years' experience. Tech Coloproctol. 2007; 11:316–322.17. De Gregorio MA, Mainar A, Tejero E, Tobio R, Alfonso E, Pinto I, et al. Acute colorectal obstruction: stent placement for palliative treatment--results of a multicenter study. Radiology. 1998; 209:117–120.18. Canon CL, Baron TH, Morgan DE, Dean PA, Koehler RE. Treatment of colonic obstruction with expandable metal stents: radiologic features. AJR Am J Roentgenol. 1997; 168:199–205.19. Rey JF, Romanczyk T, Greff M. Metal stents for palliation of rectal carcinoma: a preliminary report on 12 patients. Endoscopy. 1995; 27:501–504.20. Paul Diaz L, Pinto Pabon I, Fernandez Lobato R, Montes Lopez C. Palliative treatment of malignant colorectal strictures with metallic stents. Cardiovasc Intervent Radiol. 1999; 22:29–36.21. Yoon CJ, Song HY, Shin JH, Bae JI, Jung GS, Kichikawa K, et al. Malignant duodenal obstructions: palliative treatment using selfexpandable nitinol stents. J Vasc Interv Radiol. 2006; 17:319–326.22. Meisner S, Hensler M, Knop FK, West F, Wille-Jorgensen P. Selfexpanding metal stents for colonic obstruction: experiences from 104 procedures in a single center. Dis Colon Rectum. 2004; 47:444–450.23. Kang SG, Jung GS, Cho SG, Kim JG, Oh JH, Song HY, et al. The efficacy of metallic stent placement in the treatment of colorectal obstruction. Korean J Radiol. 2002; 3:79–86.24. Choo IW, Do YS, Suh SW, Chun HK, Choo SW, Park HS, et al. Malignant colorectal obstruction: treatment with a flexible covered stent. Radiology. 1998; 206:415–421.25. Carne PW, Frye JN, Robertson GM, Frizelle FA. Stents or open operation for palliation of colorectal cancer: a retrospective, cohort study of perioperative outcome and long-term survival. Dis Colon Rectum. 2004; 47:1455–1461.26. Bhardwaj R, Parker MC. Palliative therapy of colorectal carcinoma: stent or surgery? Colorectal Dis. 2003; 5:518–521.27. Sebastian S, Johnston S, Geoghegan T, Torreggiani W, Buckley M. Pooled analysis of the efficacy and safety of self-expanding metal stenting in malignant colorectal obstruction. Am J Gastroenterol. 2004; 99:2051–2057.28. Feretis C, Benakis P, Dimopoulos C, Georgopoulos K, Milas F, Manouras A, et al. Palliation of malignant gastric outlet obstruction with self-expanding metal stents. Endoscopy. 1996; 28:225–228.29. Pinto IT. Malignant gastric and duodenal stenosis: palliation by peroral implantation of a self-expanding metallic stent. Cardiovasc Intervent Radiol. 1997; 20:431–434.30. Bethge N, Breitkreutz C, Vakil N. Metal stents for the palliation of inoperable upper gastrointestinal stenoses. Am J Gastroenterol. 1998; 93:643–645.31. Park KB, Do YS, Kang WK, Choo SW, Han YH, Suh SW, et al. Malignant obstruction of gastric outlet and duodenum: palliation with flexible covered metallic stents. Radiology. 2001; 219:679–683.32. Jung GS, Song HY, Kang SG, Huh JD, Park SJ, Koo JY, et al. Malignant gastroduodenal obstructions: treatment by means of a covered expandable metallic stent--initial experience. Radiology. 2000; 216:758–763.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Oncological Safety of a Metallic Stent for a Left-sided Obstructive Colorectal Carcinoma
- Stent Insertion as a Bridge to One Stage Operation in Malignant Obstruction of Left Colon (6 cases)
- Self-expandable Metallic Stents for Palliative Treatment of Malignant Esophagogastric Strictures: Experiences in 103 Patients
- A Case of Pyloric Obstruction Caused by Self-expandable Metallic Stent for Palliation of Malignant Dysphagia
- A Dual Expandable Stent for Treatment of Malignant Colorectal Obstruction: Long-Term Follow-Up Results
