Intest Res.
2014 Jan;12(1):74-77. 10.5217/ir.2014.12.1.74.
Successful Treatment of Postoperative Fistula with Infliximab in a Patient with Crohn's Disease
- Affiliations
-
- 1Department of Internal Medicine, Inje University College of Medicine, Seoul, Korea. yousunk69@korea.com
- 2Department of Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2174342
- DOI: http://doi.org/10.5217/ir.2014.12.1.74
Abstract
- Nearly 80% of patients with Crohn's disease (CD) require surgical treatment for complications or failure of medical management. We managed a 31-year-old man with CD who presented with a post-operative fistula. The patient had undergone surgery due to multiple strictures and a fistula. However, a new fistula developed that connected to the intraperitoneal abscess. Intravenous antibiotics were started and multiple percutaneous drainage tubes were inserted to treat the abdominal abscess. However, the amount of drainage was consistently high, even one month after the operation. To treat the postoperative fistula, 5 mg/kg of infliximab was started, and the amount of drainage decreased dramatically to less than 10 cc a day. Some studies have reported that infliximab decreases the recurrence of CD after surgery. The effect of infliximab on post-operative fistulas in patients with CD has not been sufficiently studied. Our results indicated that the use of infliximab to treat post-operative fistula should be explored further in future clinical studies.
Keyword
MeSH Terms
Figure
-
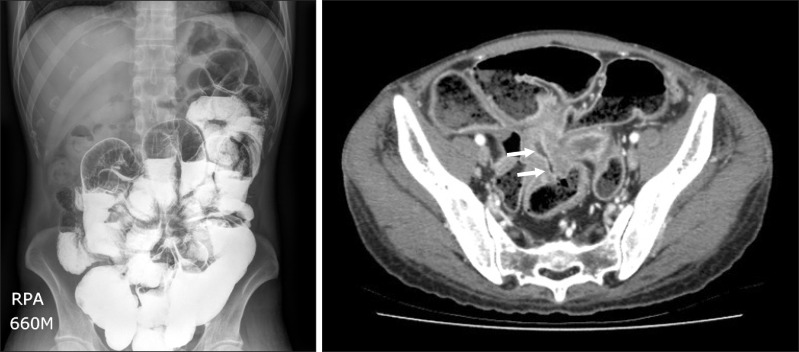
Fig. 1 Small bowel series (A) and abdominal CT scan (B) findings. They revealed ileocolic fistulas (arrows), multiple small bowel stenosis, and dilated small bowel loops with abundant fecal material.
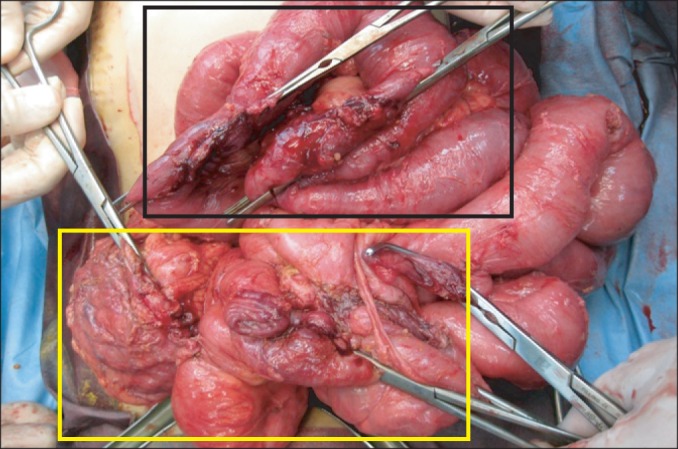
Fig. 2 Gross findings during surgery. Ileocecectomy, rectal repair (yellow square), and small bowel and sigmoid resection (black square) were performed.
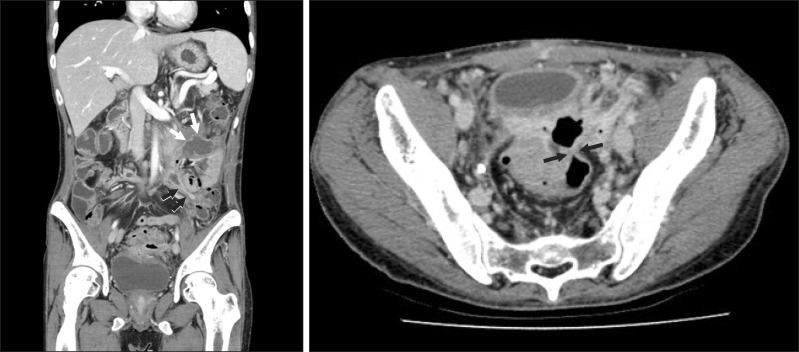
Fig. 3 Postoperative abdominal CT scan. It showed a fistula (black arrows) and intraperitoneal abscess (white arrows), which needed percutaneous drainage (A: coronal view, B: axial view).
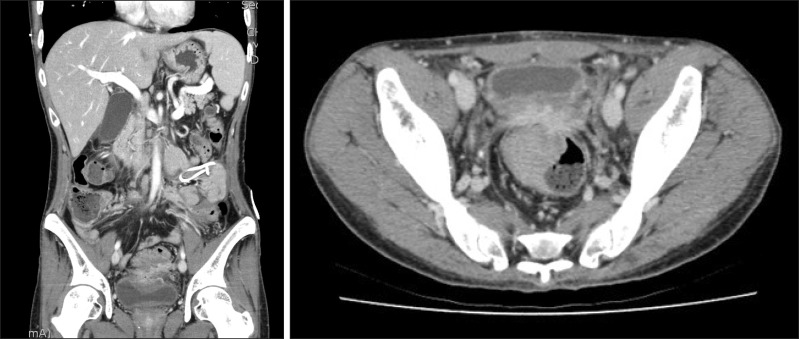
Fig. 4 The follow-up abdominal CT findings. The abscess and fistula disappeared (A: coronal view, B: axial veiw).
Reference
-
1. Olaison G, Sjodahl R, Tagesson C. Glucocorticoid treatment in ileal Crohn's disease: relief of symptoms but not of endoscopically viewed inflammation. Gut. 1990; 31:325–328. PMID: 2323598.2. Gardiner KR, Dasari BV. Operative management of small bowel Crohn's disease. Surg Clin North Am. 2007; 87:587–610. PMID: 17560414.
Article3. Yamamoto T. Factors affecting recurrence after surgery for Crohn's disease. World J Gastroenterol. 2005; 11:3971–3979. PMID: 15996018.
Article4. Thia KT, Loftus EV Jr, Sandborn WJ, Yang SK. An update on the epidemiology of inflammatory bowel disease in Asia. Am J Gastroenterol. 2008; 103:3167–3182. PMID: 19086963.
Article5. Lindhagen T, Ekelund G, Leandoer L, Hildell J, Lindstrom C, Wenckert A. Pre- and post-operative complications in Crohn's disease with special reference to duration of preoperative disease history. Scand J Gastroenterol. 1984; 19:194–203. PMID: 6719032.
Article6. Post S, Betzler M, von Ditfurth B, Schurmann G, Kuppers P, Herfarth C. Risks of intestinal anastomoses in Crohn's disease. Ann Surg. 1991; 213:37–42. PMID: 1985536.7. Subramanian V, Saxena S, Kang JY, Pollok RC. Preoperative steroid use and risk of postoperative complications in patients with inflammatory bowel disease undergoing abdominal surgery. Am J Gastroenterol. 2008; 103:2373–2381. PMID: 18616660.
Article8. Nielsen OH, Rogler G, Hahnloser D, Thomsen OØ. Diagnosis and management of fistulizing Crohn's disease. Nat Clin Pract Gastroenterol Hepatol. 2009; 6:92–106. PMID: 19153563.
Article9. Miehsler W, Reinisch W, Kazemi-Shirazi L, et al. Infliximab: lack of efficacy on perforating complications in Crohn's disease. Inflamm Bowel Dis. 2004; 10:36–40. PMID: 15058525.10. Appau KA, Fazio VW, Shen B, et al. Use of infliximab within 3 months of ileocolonic resection is associated with adverse postoperative outcomes in Crohn's patients. J Gastrointest Surg. 2008; 12:1738–1744. PMID: 18709420.
Article11. Marchal L, D'Haens G, Van Assche G, et al. The risk of post-operative complications associated with infliximab therapy for Crohn's disease: a controlled cohort study. Aliment Pharmacol Ther. 2004; 19:749–754. PMID: 15043515.12. Ye BD, Yang SK, Shin SJ, et al. Guidelines for the management of Crohn's disease. Intest Res. 2012; 10:26–66.
Article13. Sorrentino D, Paviotti A, Terrosu G, Avellini C, Geraci M, Zarifi D. Low-dose maintenance therapy with infliximab prevents postsurgical recurrence of Crohn's disease. Clin Gastroenterol Hepatol. 2010; 8:591–599.e1. PMID: 20139033.
Article14. Regueiro M, Schraut W, Baidoo L, et al. Infliximab prevents Crohn's disease recurrence after ileal resection. Gastroenterology. 2009; 136:441–450.e1. PMID: 19109962.
Article15. Sorrentino D, Terrosu G, Avellini C, Beltrami CA, Bresadola V, Toso F. Prevention of postoperative recurrence of Crohn's disease by infliximab. Eur J Gastroenterol Hepatol. 2006; 18:457–459. PMID: 16538123.
Article16. Yang SK, Yun S, Kim JH, et al. Epidemiology of inflammatory bowel disease in the Songpa-Kangdong district, Seoul, Korea, 1986-2005: a KASID study. Inflamm Bowel Dis. 2008; 14:542–549. PMID: 17941073.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Factors Affecting Surgical Treatment With Infliximab Therapy in Perianal Fistula With Crohn Disease
- Adalimumab or infliximab: which is better for perianal fistula in Crohn's disease?
- Recent Trends of Infliximab Treatment for Crohn's Disease
- Clinical Outcome of a Rectovaginal Fistula in Crohn's Disease
- Clinical efficacy of adalimumab versus infliximab and the factors associated with recurrence or aggravation during treatment of anal fistulas in Crohn's disease
