The Development of Medical Record Items: a User-centered, Bottom-up Approach
- Affiliations
-
- 1Department of Medical Informatics, Yonsei University Healthcare System, Seoul, Korea.
- 2Department of Cardiovascular Surgery, Yonsei University College of Medicine, Seoul, Korea.
- 3Biomedical Knowledge Engineering Lab, Seoul National University, Seoul, Korea.
- 4Department of Plastic and Reconstructive Surgery, Yonsei University College of Medicine, Seoul, Korea. SGM625@yuhs.ac
- KMID: 2166613
- DOI: http://doi.org/10.4258/hir.2012.18.1.10
Abstract
OBJECTIVES
Clinical documents (CDs) have evolved from traditional paper documents containing narrative text information into the electronic record sheets composed of itemized records, where each record is expressed as an item with a specific value. We defined medical record (MR) items to be information entities with a specific value. These entities were then used to compile form-based clinical documents as part of an electronic health record system (EHR-s).
METHODS
We took a reusable bottom-up developmental approach for the MR items, which provided three things: efficient incorporation of the local needs and requirements of the medical professionals from various departments in the hospital, comprehensive inclusion of the essential concepts of the basic elements required in clinical documents, and the provision of a structured means for meaningful data entry and retrieval. This paper delineates our experiences in developing and managing medical records at a large tertiary university hospital in Korea.
RESULTS
We collected 63,232 MR items from paper records scanned into 962 CDs. The MR item database was constructed using 13,287 MR items after removing redundant items. During the first year of service users requested changes to be made to 235 (1.8%) attributes of the MR items and also requested the additional 9,572 new MR items. In the second year, the attributes of 70 (0.5%) of the existing MR items were changed and 3,704 new items were added. The number of registered MR items increased by 72.0% in the first year and 27.9% in the second year.
CONCLUSIONS
The MR item concept provides an easier and more structured means of data entry within an EHR-s. By using these MR items, various kinds of clinical documents can be easily constructed and allows for medical information to be reused and retrieved as data. The success of the use of MR items in a large tertiary university hospital system provides evidence that verifies our approach as being an efficient means of user-oriented and structured data entry, enabling the easy reuse of medical records.
Keyword
Figure
-
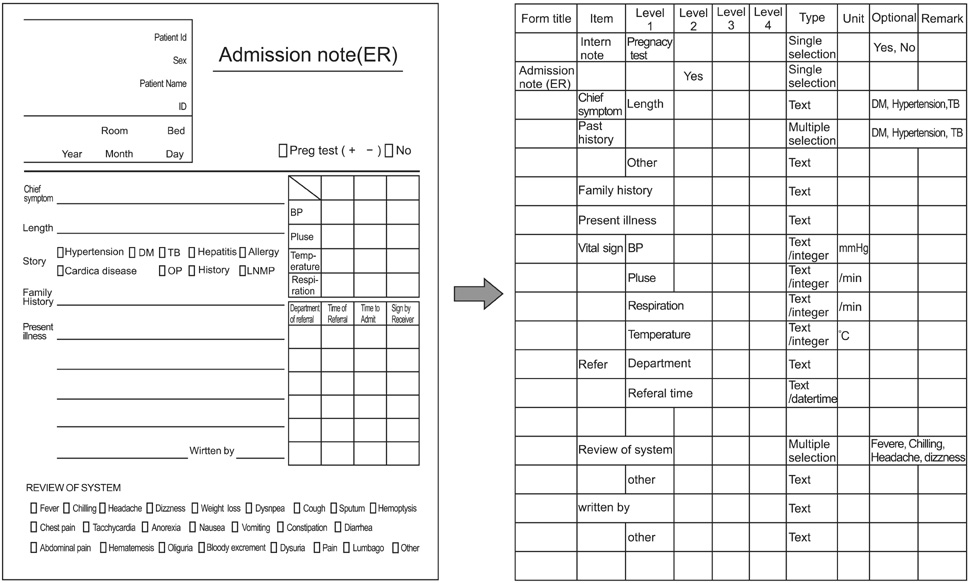
Figure 1 Hierarchical list of medical record items.
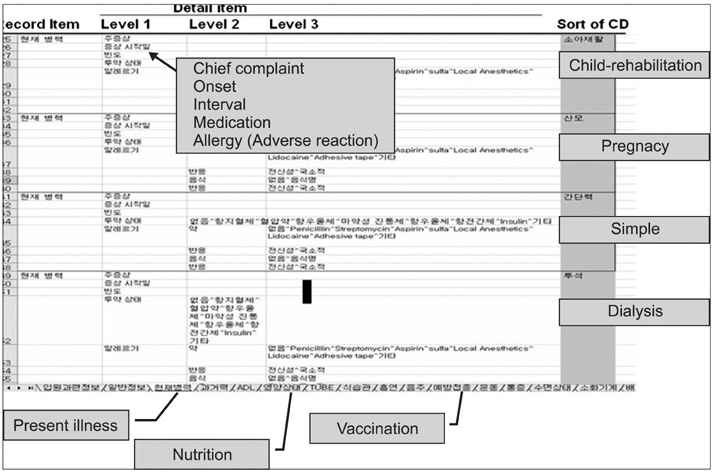
Figure 2 Similarity or identity checking.
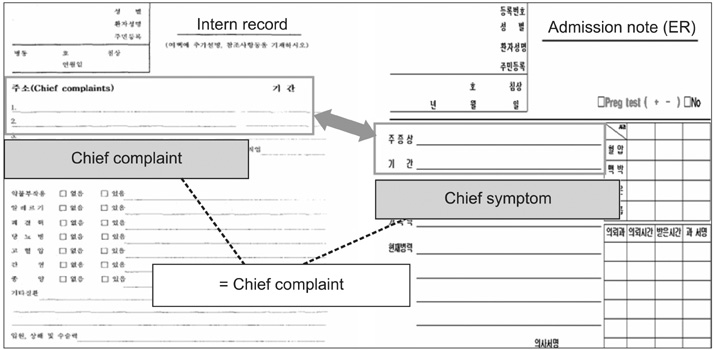
Figure 3 Merge of redundant medical record items into a single item.
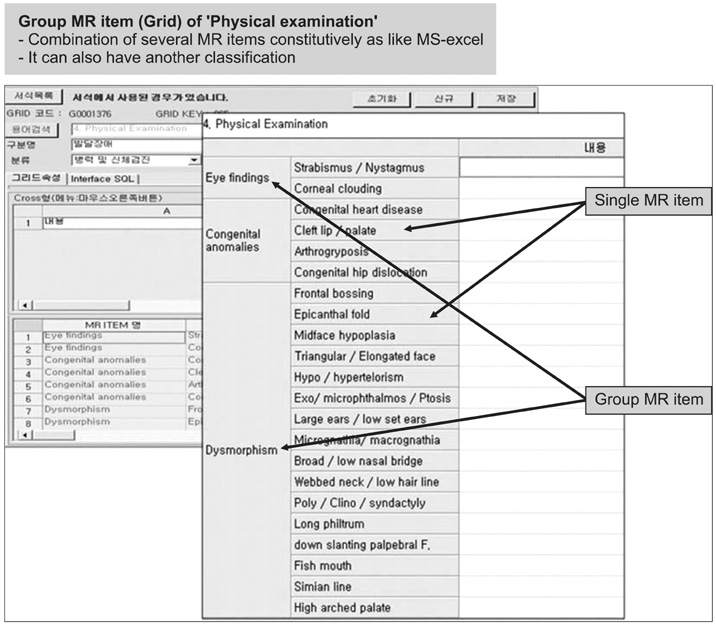
Figure 4 Grid arrangement. MR: medical record.
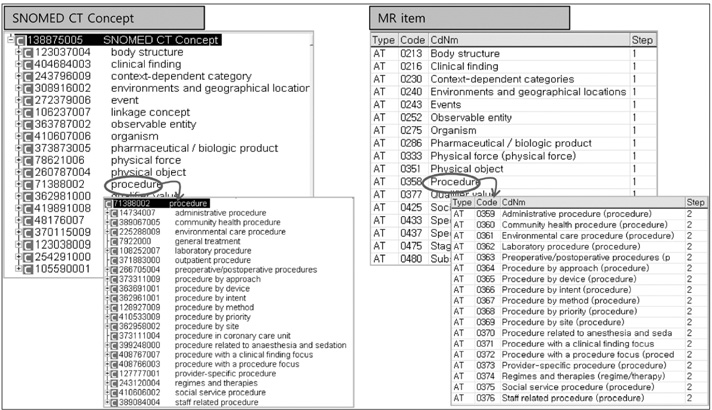
Figure 5 Systematized Nomenclature of Medicine (SNOMED) and terminology attributes.
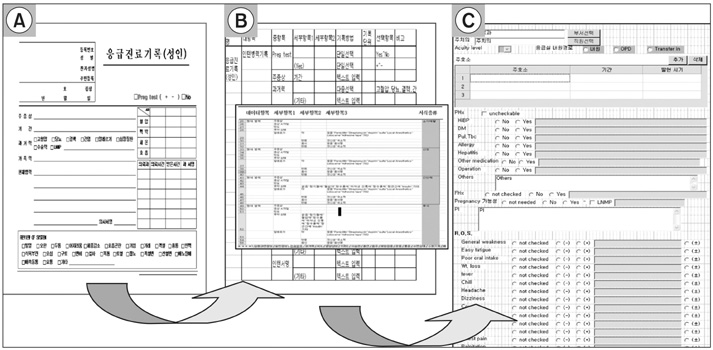
Figure 6 Creation of electronic clinical documents. (A) Paper-based clinical document, (B) collection of medical record items and definition of attribute, (C) clinical document.

Figure 7 Changes in medical record items over time.
Cited by 1 articles
-
Reusability of EMR Data for Applying Cubbin and Jackson Pressure Ulcer Risk Assessment Scale in Critical Care Patients
Eunkyung Kim, Mona Choi, JuHee Lee, Young Ah Kim
Healthc Inform Res. 2013;19(4):261-270. doi: 10.4258/hir.2013.19.4.261.
Reference
-
1. Eduljee A, Rocha RA. Practical evaluation of clinical guideline document models. AMIA Annu Symp Proc. 2003. 836.2. Soto CM, Kleinman KP, Simon SR. Quality and correlates of medical record documentation in the ambulatory care setting. BMC Health Serv Res. 2002. 2:22.
Article3. Tully MP, Cantrill JA. Insights into creation and use of prescribing documentation in the hospital medical record. J Eval Clin Pract. 2005. 11:430–437.
Article4. The World Wide Web Consortium (W3C). Extensible markup language (XML) 1.0. 1998. Cambridge (MA): W3C;Technical report no.: REC-xml-19980210.5. Elkin PL, Brown SH, Husser CS, Bauer BA, Wahner-Roedler D, Rosenbloom ST, Speroff T. Evaluation of the content coverage of SNOMED CT: ability of SNOMED clinical terms to represent clinical problem lists. Mayo Clin Proc. 2006. 81:741–748.
Article6. Wasserman H, Wang J. An applied evaluation of SNOMED CT as a clinical vocabulary for the computerized diagnosis and problem list. AMIA Annu Symp Proc. 2003. 699–703.7. Elevitch FR. SNOMED CT: electronic health record enhances anesthesia patient safety. AANA J. 2005. 73:361–366.8. Nash SK. Nonsynonymous synonyms: correcting and improving SNOMED CT. AMIA Annu Symp Proc. 2003. 949.9. Herbert I, Hawking M. Bringing SNOMED-CT into use within primary care. Inform Prim Care. 2005. 13:61–64.
Article10. Elkin PL, Brown SH, Carter J, Bauer BA, Wahner-Roedler D, Bergstrom L, Pittelkow M, Rosse C. Guideline and quality indicators for development, purchase and use of controlled health vocabularies. Int J Med Inform. 2002. 68:175–186.
Article11. Elkin PL, Brown SH, Lincoln MJ, Hogarth M, Rector A. A formal representation for messages containing compositional expressions. Int J Med Inform. 2003. 71:89–102.
Article12. Dolin RH, Alschuler L, Beebe C, Biron PV, Boyer SL, Essin D, Kimber E, Lincoln T, Mattison JE. The HL7 clinical document architecture. J Am Med Inform Assoc. 2001. 8:552–569.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Development of a User Centered Web Site for Mental Health Management in Adolescents
- Study on User Interface of Pathology Picture Archiving and Communication System
- Factors affecting the users'satisfaction on the electronic medical record system
- Estimating Cognitive Load in a Mobile Personal Health Record Application: A Cognitive Task Analysis Approach
- Comparison of Open-Source Electronic Health Record Systems Based on Functional and User Performance Criteria
