Korean J Neurotrauma.
2013 Oct;9(2):69-73. 10.13004/kjnt.2013.9.2.69.
Clinical Experiences of Unruptured Vertebral Artery Dissection
- Affiliations
-
- 1Department of Neurosurgery, Guri Hospital, College of Medicine, Hanyang University, Guri, Korea. cjh2324@hanyang.ac.kr
- KMID: 2156103
- DOI: http://doi.org/10.13004/kjnt.2013.9.2.69
Abstract
OBJECTIVE
The natural course of unruptured vertebral artery dissection remains unclear. The clinical manifestation of unruptured vertebral artery dissection varies from headache, focal neurologic deficits caused by ischemia to subarachnoid hemorrhage with high mortality. The purpose of this study is to investigate the clinical course of unruptured vertebral artery dissection.
METHODS
From March 2011 to April 2013, 7 patients with headache or nuchal pain by spontaneous vertebral artery dissection visited our institute were retrospectively reviewed. Their clinical data was obtained by medical records and radiologic studies including computed tomographic angiography, magnetic resonance imaging, magnetic resonance angiography and digital subtraction angiography.
RESULTS
No patient experienced fatal outcome by subarachnoid hemorrhage or vertebrobasilar ischemia during follow-up period. Radiologic studies also did not show the evidence of subarachnoid hemorrhage or vertebrobasilar ischemia. Follow-up angiography showed the decreased size or disappearance of aneurysm in 3 patients.
CONCLUSION
This study suggests that the natural course of unruptured vertebral artery dissection is not aggressive. Patients with unruptured vertebral artery dissection could be managed with conservative treatment including anticoagulants and/or antiplatelet agents.
MeSH Terms
-
Aneurysm
Aneurysm, Dissecting
Angiography
Anticoagulants
Fatal Outcome
Follow-Up Studies
Headache
Humans
Ischemia
Magnetic Resonance Angiography
Magnetic Resonance Imaging
Medical Records
Mortality
Neurologic Manifestations
Platelet Aggregation Inhibitors
Retrospective Studies
Subarachnoid Hemorrhage
Vertebral Artery Dissection*
Vertebral Artery*
Vertebrobasilar Insufficiency
Anticoagulants
Platelet Aggregation Inhibitors
Figure
-
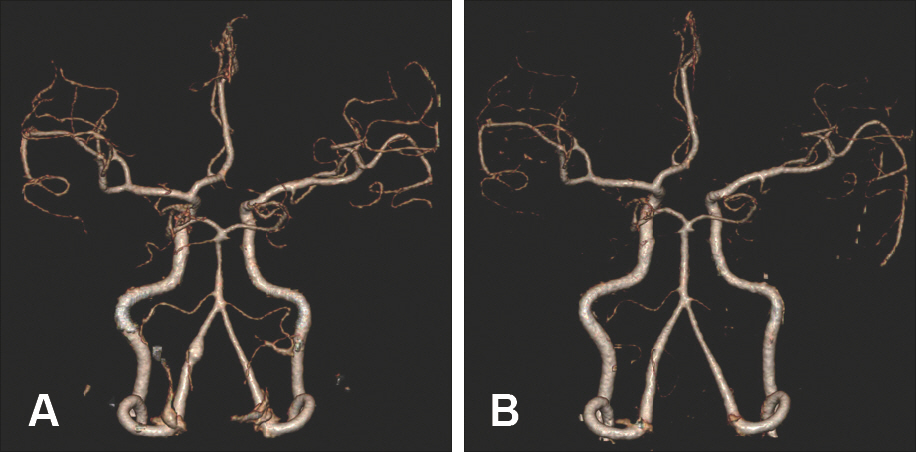
FIGURE 1. Case 2. A 54-year-old woman with intermittent headache after swimming. A: Initial CTA showing fusiform aneurysm at left V4 segment. B: After 4 months, the aneurysm disappeared completely. CTA: computed tomographic angiography.
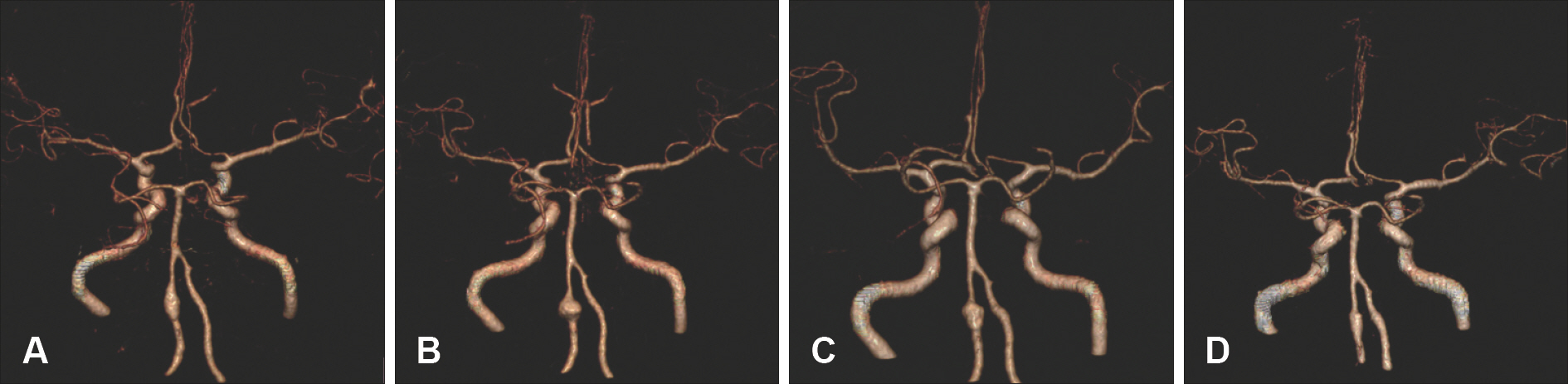
FIGURE 2. Case 4. A 56-year-old male with headache after a physical fight. A: Initial CTA showing fusiform aneurysm at left distal vertebral artery. B: After 5 months, increase in size and change in shape of the aneurysm from fusiform to globular. C: One month later, size of the aneurysm decreased reversely and its shape changed from globular to fusiform. D: The recent CTA, aneurysm became smaller. CTA: computed tomographic angiography.
Reference
-
References
1. Aoki N, Sakai T. Rebleeding from intracranial dissecting aneurysm in the vertebral artery. Stroke. 21:1628–1631. 1990.
Article2. Auer RN, Krcek J, Butt JC. Delayed symptoms and death after minor head trauma with occult vertebral artery injury. J Neurol Neurosurg Psychiatry. 57:500–502. 1994.
Article3. Broom ND, Ramsey G, Mackie R, Martin BJ, Stehbens WE. A new biomechanical approach to assessing the fragility of the internal elastic lamina of the arterial wall. Connect Tissue Res. 30:143–155. 1993.
Article4. Hayes WT, Bernhardt H, Young JM. Fusiform arteriosclerotic aneurysm of the basilar artery. Five cases including two ruptures. Vasc Surg. 1:171–178. 1967.5. Hosoya T, Adachi M, Yamaguchi K, Haku T, Kayama T, Kato T. Clinical and neuroradiological features of intracranial vertebrobasilar artery dissection. Stroke. 30:1083–1090. 1999.
Article6. Ishikawa T, Nakamura N, Houkin K, Nomura M. Pathological consideration of a “blister-like” aneurysm at the superior wall of the internal carotid artery: case report. Neurosurgery. 40:403–405. ; discussion 405–406,. 1997.
Article7. Kai Y, Nishi T, Watanabe M, Morioka M, Hirano T, Yano S, et al. Strategy for treating unruptured vertebral artery dissecting aneurysms. Neurosurgery. 69:1085–1091. ;discussion 1091–1092,. 2011.
Article8. Kim CH, Son YJ, Paek SH, Han MH, Kim JE, Chung YS, et al. Clinical analysis of vertebrobasilar dissection. Acta Neurochir (Wien). 148:395–404. 2006.
Article9. Kitanaka C, Tanaka J, Kuwahara M, Teraoka A, Sasaki T, Takakura K, et al. Nonsurgical treatment of unruptured intracranial vertebral artery dissection with serial follow-up angiography. J Neurosurg. 80:667–674. 1994.
Article10. Masawa N, Glagov S, Zarins CK. Quantitative morphologic study of intimal thickening at the human carotid bifurcation: II. The compensatory enlargement response and the role of the intima in tensile support. Atherosclerosis. 107:147–155. 1994.
Article11. Mizutani T. Natural course of intracranial arterial dissections. J Neurosurg. 114:1037–1044. 2011.
Article12. Mizutani T, Aruga T, Kirino T, Miki Y, Saito I, Tsuchida T. Recurrent subarachnoid hemorrhage from untreated ruptured vertebrobasilar dissecting aneurysms. Neurosurgery. 36:905–911. ; discussion 912–913,. 1995.
Article13. Mizutani T, Kojima H, Asamoto S. Healing process for cerebral dissecting aneurysms presenting with subarachnoid hemorrhage. Neurosurgery. 54:342–347. ; discussion 347–348,. 2004.
Article14. Mokri B, Houser OW, Sandok BA, Piepgras DG. Spontaneous dissections of the vertebral arteries. Neurology. 38:880–885. 1988.
Article15. Naito I, Iwai T, Sasaki T. Management of intracranial vertebral artery dissections initially presenting without subarachnoid hemorrhage. Neurosurgery. 51:930–937. ; discussion 937–938,. 2002.
Article16. Nass R, Hays A, Chutorian A. Intracranial dissecting aneurysms in childhood. Stroke. 13:204–207. 1982.
Article17. Pozzati E, Padovani R, Fabrizi A, Sabattini L, Gaist G. Benign arterial dissections of the posterior circulation. J Neurosurg. 75:69–72. 1991.
Article18. Ramgren B, Cronqvist M, Romner B, Brandt L, Holtås S, Larsson EM. Vertebrobasilar dissection with subarachnoid hemorrhage: a retrospective study of 29 patients. Neuroradiology. 47:97–104. 2005.
Article19. Sakata N, Takebayashi S, Kojima M, Masawa N, Suzuki K, Takata-ma M, et al. Different roles of arteriosclerosis in the rupture of intracranial dissecting aneurysms. Histopathology. 38:325–337. 2001.
Article20. Sasaki O, Ogawa H, Koike T, Koizumi T, Tanaka R. A clinicopathological study of dissecting aneurysms of the intracranial vertebral artery. J Neurosurg. 75:874–882. 1991.
Article21. Schievink WI. Spontaneous dissection of the carotid and vertebral arteries. N Engl J Med. 344:898–906. 2001.
Article22. Tsutsumi M, Kawano T, Kawaguchi T, Kaneko Y, Ooigawa H. Dissecting aneurysm of the vertebral artery causing subarachnoid hemorrhage after non-hemorrhagic infarction–case report. Neurol Med Chir (Tokyo). 40:628–631. 2000.23. Willis BK, Greiner F, Orrison WW, Benzel EC. The incidence of vertebral artery injury after midcervical spine fracture or subluxation. Neurosurgery. 34:435–441. ; discussion 441–442,. 1994.
Article24. Yoshimoto Y, Wakai S. Unruptured intracranial vertebral artery dissection. Clinical course and serial radiographic imagings. Stroke. 28:370–374. 1997.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Simultaneous Vertebral Artery Dissection and Contralateral Posterior Inferior Cerebellar Artery Dissecting Aneurysm
- High-Resolution Magnetic Resonance Imaging of Intracranial Vertebral Artery Dissecting Aneurysm for Planning of Endovascular Treatment
- Locked-in Syndrome Performed Endovascular Treatment for Vertebral Artery Dissection and Basilar Artery Occlusion Caused by a Golf Swing
- Vertebral Artery Dissection Presenting as Transient Global Amnesia: A Case Report and Review of Literature
- Endovascular Treatment Strategies for Vertebral Artery Dissection: A Single-Center Experience and Literature Review
