A Novel Concept for the Best Coronal Alignment of Pedicle Screws in Multilevel Lumbar Posterior Instrumentation - A Technical Note
- Affiliations
-
- 1Department of Orthopaedic Surgery, Asan Medical Center College of Medicine, University of Ulsan, Seoul, Korea. cslee@amc.seoul.kr
- 2Department of Orthopaedic Surgery, Pusan Paik Hospital College of Medicine, Inje University, Pusan, Korea.
- 3Department of Orthopaedic Surgery, National Police Hospital, Korea.
- KMID: 2097838
- DOI: http://doi.org/10.4184/jkss.2008.15.2.96
Abstract
- Correct alignment of pedicle screws is imperative in multilevel instrumentation. However, there has been no report addressing the technical aspects of this subject. If the head diameter of a pedicle screw is D, the head height is H, and the convergence angle of the screw being inserted is alpha, then the distance between the extension line of the medial borders of the inserted screw heads and the insertion point of the adjacent screw (A) is described by the following formula: A = 1/2Dcos alpha- Hsin alpha If an L3 pedicle screw (D=13 mm, H=15 mm) is to be inserted with a convergence angle of 14 degrees after the insertion of L4 and L5 screws, its insertion point should be 3.6 mm medial to the extension line of the centers of the L4 and L5 screws and 2.7 mm lateral to the extension line of their medial borders for all screw heads, so it can be aligned in the coronal plane. In order to achieve the best alignment, a pedicle screw is inserted between the extended line of the centers and that of the medial borders of the inserted adjacent screw heads. For the routine range of convergence angles, it is essential to move the entry point medially toward the extended line connecting the medial borders of the inserted adjacent screw heads.
MeSH Terms
Figure
-
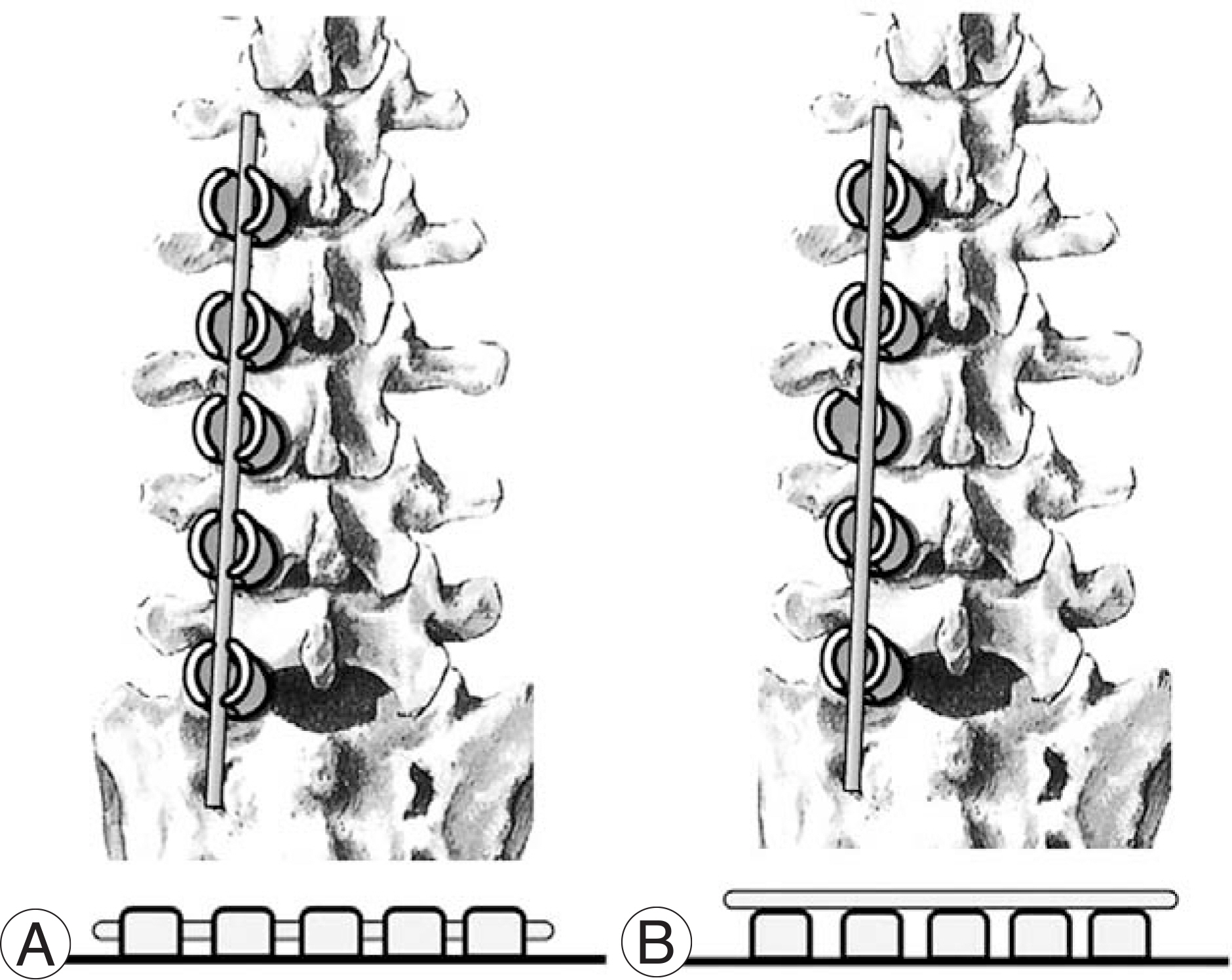
Fig. 1. If screw heads are not correctly aligned, rod insertion could be difficult (bottom, B). (A) The best alignment, (B) An inappropriate alignment.
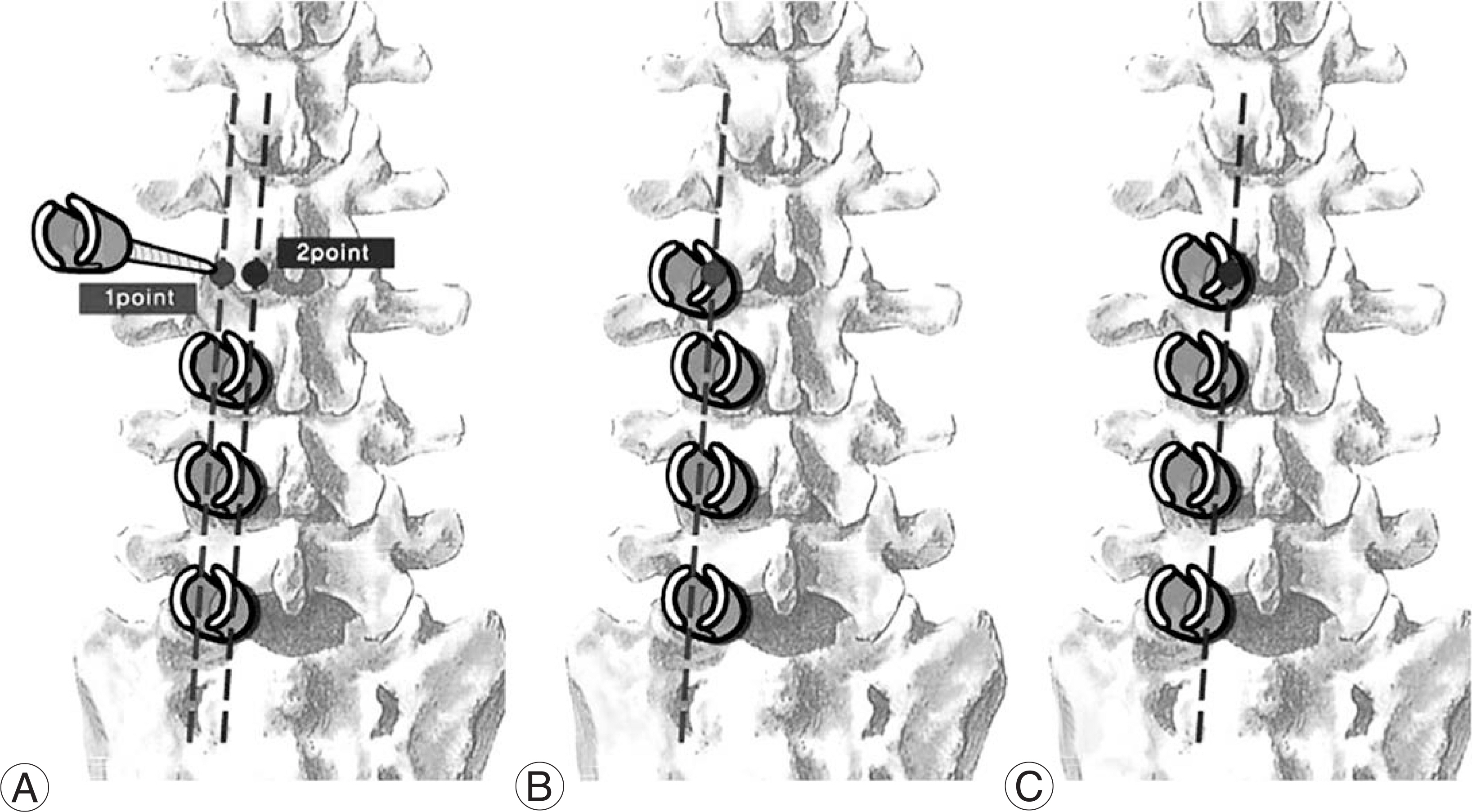
Fig. 2. (A) The first point is located in the extended line connecting the centers of adjacent screw heads (red), and the second point is in the extended line connecting their medial borders (blue). (B) The screw being inserted was lateralized. (C) The best coronal alignment was obtained.

Fig. 3. Relationship between the base (adjacent) screw and the screw that will be inserted. (A) If a pedicle screw is directed in line with the center of the base screw head, it will be lateralized in coronal plane. (B) The entry point must be located in line with the medial border of the base screw head to get the best alignment of screw heads in coronal plane. These schemas demonstrate the same situations as B and C in figure 2, respectively.
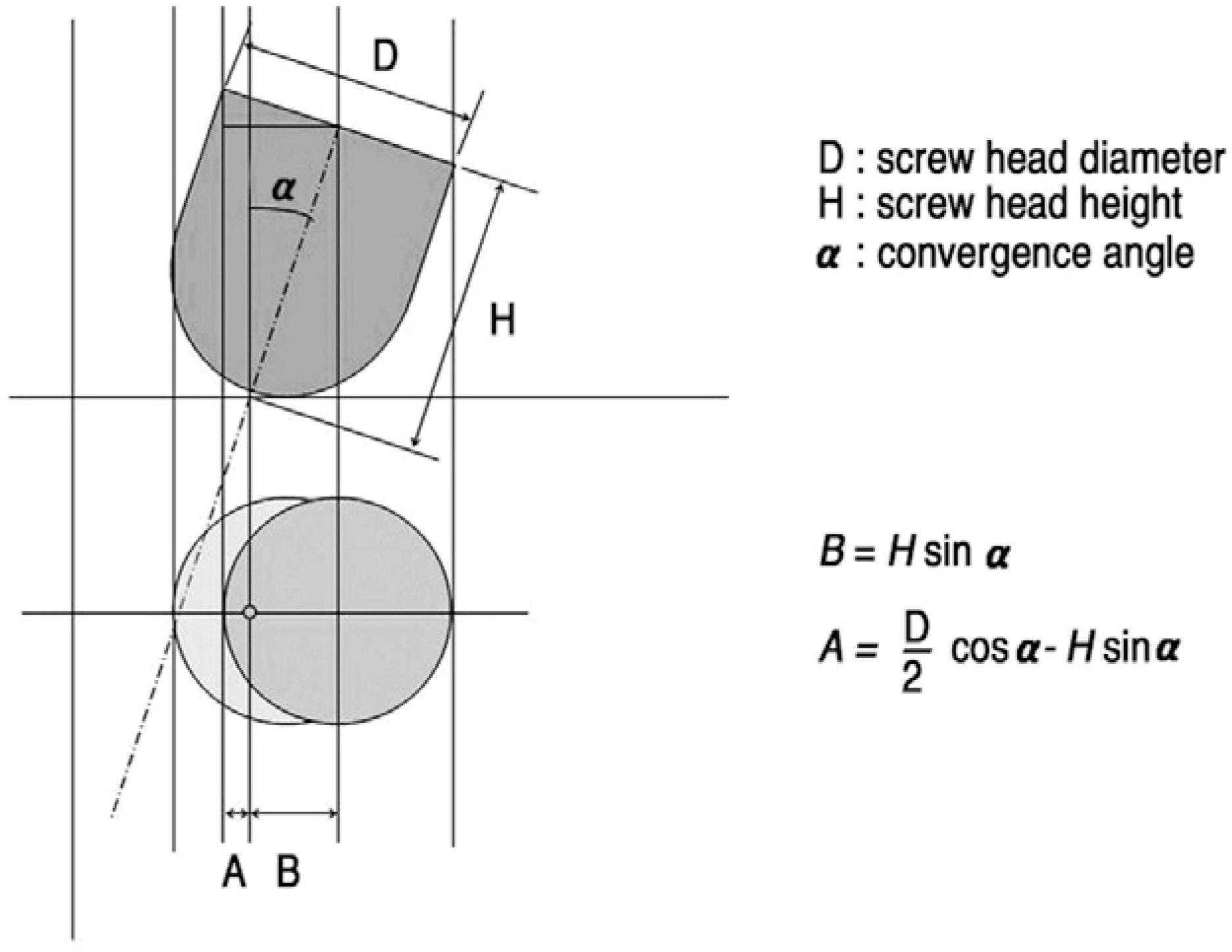
Fig. 4. The suggested numerical formula describes the distances between the entry point and the medial border (A) and the center (B) of a screw head, respectively.
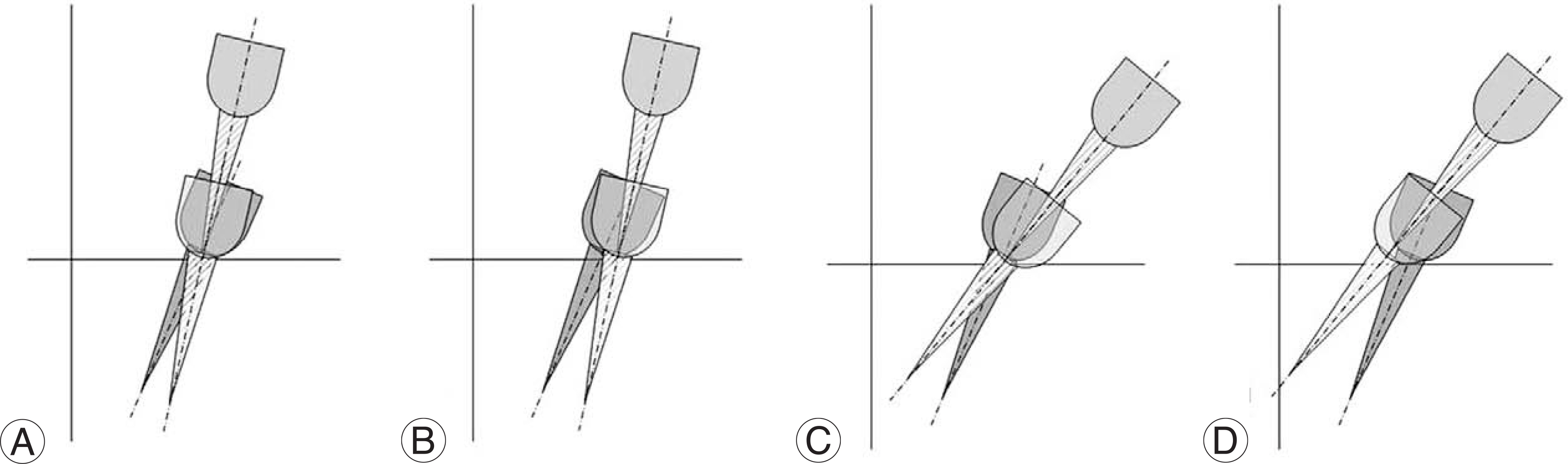
Fig. 5. Adjustment of entry point according to convergence angle. The entry point should be slightly lateralized in case that the convergence angle is smaller than that of a base (adjacent) screw to align the screw heads (A, B). If the convergence angle of a screw being inserted is larger than that of a base (adjacent) screw, its entry point must be slightly medialized (C, D).
Reference
-
1). Zindrick MR, Wiltse LL, Doornik A, et al. Analysis of the morphometric characteristics of the thoracic and lumbar pedicles. Spine. 1987; 12:160–166.
Article2). Suk SI, Kim WJ, Lee SM, Kim JH, Chung ER. Thoracic pedicle screw fixation in spinal deformities. Spine. 2001; 26:2049–2057.
Article3). Park HJ, Rha JH, Lee DH. Entry point of pedicle screw in the lumbar spine. J Korean Soc Spine Surg. 1999; 6:349–354.4). Krag MH. Biomechanics of thoracolumbar spinal fixation. Spine. 1991; 16:84–99.
Article5). Magerl FP. Stabilization of the lower thoracic and lumbar spine with external skeletal fixation. Clin Orthop. 1984; 189:125–141.
Article6). Roy-Camille R, Saillant G, Mazel C. Internal fixation of the lumbar spine with pedicle screw plating, Clin Orthop. 1986; 203:7–17.7). Ebraheim NA, Xu R, Darwich M, Yeasting RA. Anatomic relation between the lumbar pedicle and the adjacent neural structures. Spine. 1997; 22:2338–2341.8). Attar A, Ugur HC, Uz A, Tekdemir I, Egemen N, Genc Y. Lumbar pedicle: surgical anatomic evaluation and relationships. Eur spine J. 2001; 10:10–15.
Article9). Soyuncu Y, Yildirim FB, Sekban H, Ozdemir H, Akyildiz F, Sindel M. Anatomic evaluation and relationship between the lumbar pedicle and adjacent neural structures. J Spinal Disord Tech. 2005; 18:243–246.10). Stanford RE, Loefler AH, Stanford PM, Walsh WR. Multiaxial pedicle screw designs: Static and dynamic mechanical testing. Spine. 2004; 29:367–375.
Article11). Shepard MF, Davies MR, Abayan A, Kabo JM, Wang JC. Effects of polyaxial pedicle screws on lumbar construct rigidity. J Spinal Disord Tech. 2002; 15:233–236.
Article12). Kuklo TR, Potter BK, Polly DW, Lenke LG. Monaxial versus multiaxial thoracic pedicle screws in the correction of adolescent idiopathic scoliosis. Spine. 2005; 30:2113–2120.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Biomechanical Comparison of Multilevel Stand-Alone Lumbar Lateral Interbody Fusion With Posterior Pedicle Screws: An In Vitro Study
- Bilateral Pedicle and Crossed Translaminar Screws in C2
- Does the Addition of a Dynamic Pedicle Screw to a Fusion Segment Prevent Adjacent Segment Pathology in the Lumbar Spine?
- Change of Kyphotic Angle in Posterior Pedicle Screw Fixation for Thoracic and Lumbar Burst Fractures: Comparison Study by the Screw Fixation Level
- Segmental pedicle screw fixation in the treatment of Thoracic idiopathic scoliosis
