Surgical Treatment of Kummell Disease with Neurologic Deficits: Posterolateral Decompression and Posterior Reconstruction
- Affiliations
-
- 1Department of Orthopaedic Surgery, School of Medicine, Kyung Hee University, Seoul, Korea. ktkim@khmc.or.kr
- KMID: 2097753
- DOI: http://doi.org/10.4184/jkss.2001.8.2.136
Abstract
-
STUDY DESIGN: Retrospective study was performed in eight patients with Kummell disease.
OBJECTIVES
To access the results of posterolateral decompression and posterior reconstruction in Kummell disease with neurologic deficits. SUMMARY OF LITERATURE REVIEW: Severe osteoporosis is the most frequent cause of spinal compression fracture. Vertebral compression fracture in senile osteoporosis is characterized by the late development and slow progression of paraplegia. When conservative treatment for paraplegia proves ineffective, an early operation is recommended.
MATERIALS AND METHODS
From June 1996 to February 2000, eight consecutive Kummell disease patients with neurologic deficits underwent posterolateral decompression and posterior reconstruction. We analyzed operation time, loss of blood through the medical records. Change of segmental kyphotic angle, bone union were assessed by plain radiographs, the clinical results were analyzed according to changes of pain and neurological status.
RESULTS
Mean operation time was 217 minutes, mean bleeding loss was 682 ml. The mean preoperative segmental kyphotic angle measured 22.6 degrees, and decreased to 4.4 degrees at postoperative evaluation, and 6.8 degrees at final follow-up. Bony union was obtained in 9 months. At preoperative time, four cases showed Frankel grade C and four cases Frankel grade D. At last follow-up time, one case Frankel grade D and six cases Frankel grade E.
CONCLUSIONS
We concluded that posterolateral decompression and posterior reconstruction is a useful method for the treatment of Kummell disease with neurologic deficits.
MeSH Terms
Figure
-

Fig. 1. Posterolateral decompression through pedicle. Fig. A. Removal of medial part of both pedicles. Fig. B. Curettage of cancellous bone. Fig. C. Pushing the thin cortical shell anteriorly by curved curette. Fig. D. Impacted bone graft was done with autogenous and allogenous bone. Fig. E. Connection of rod to the pedicle screws.
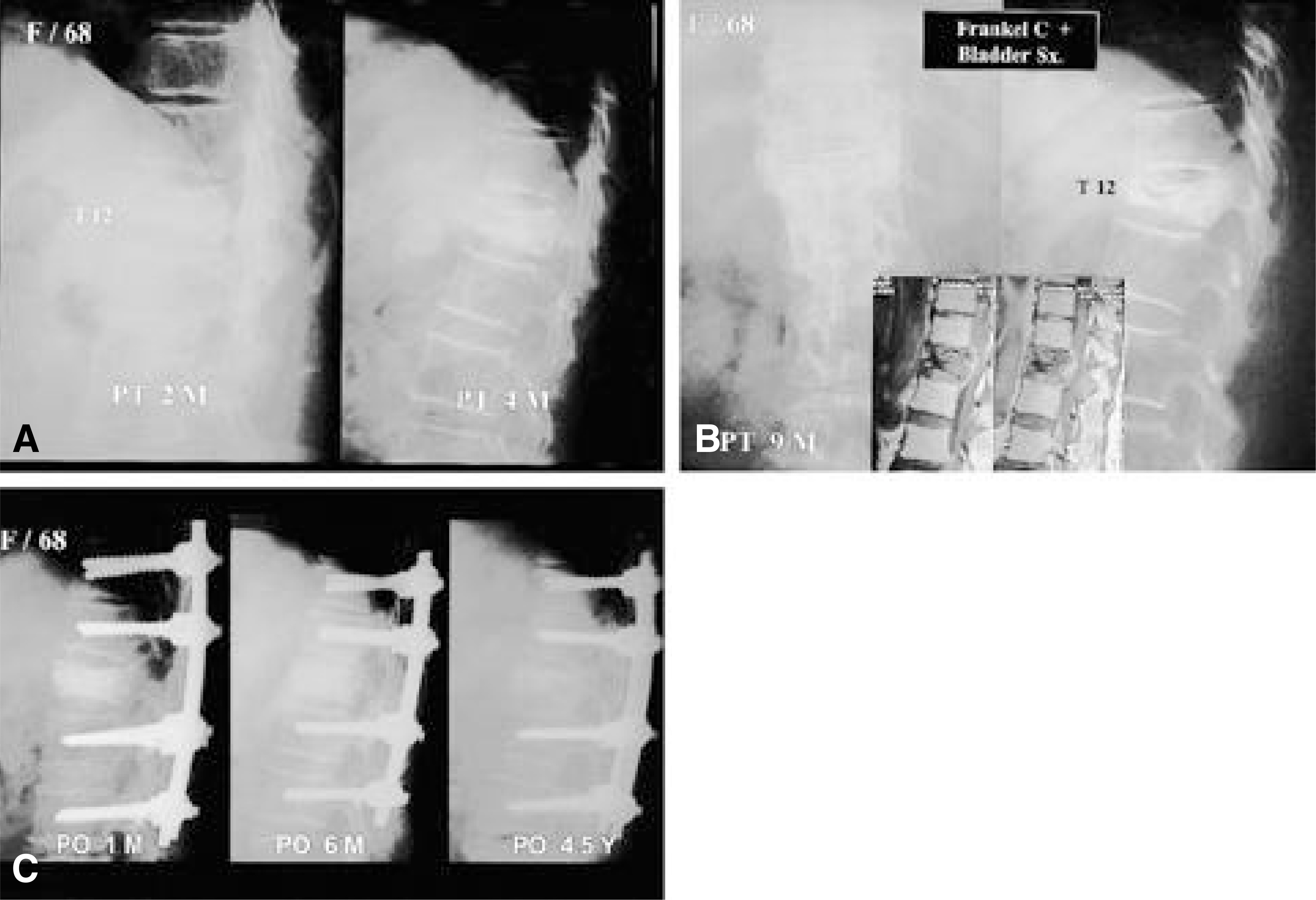
Fig. 2-A. Thoracolumbar spine lateral radiography of a 68-year-old woman shows compression fracture of T12. Fig. 2-B. Nine months followup lateral radiography and MRI shows collapse of T12 and spinal cord compression. Fig. 2-C. Postoperatively, reconstructed spine is good align-ment and complete bone union.
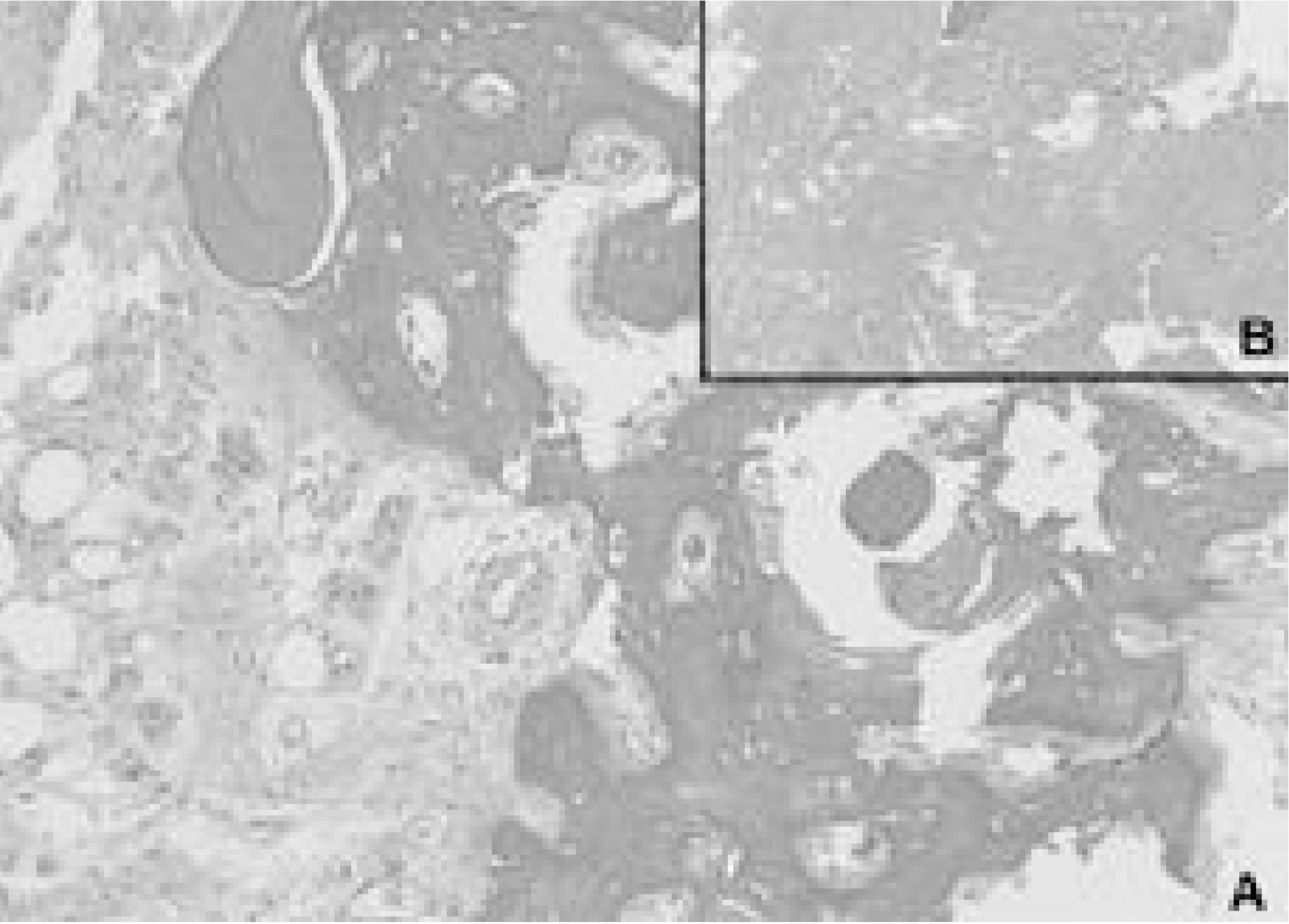
Fig. 3-A. Histological examination shows apposition of newly formed “woven bone” on preexisting lamellar bone. Fig. 3-B. Granulation tissue and necrotic tissue is seen around the callus.
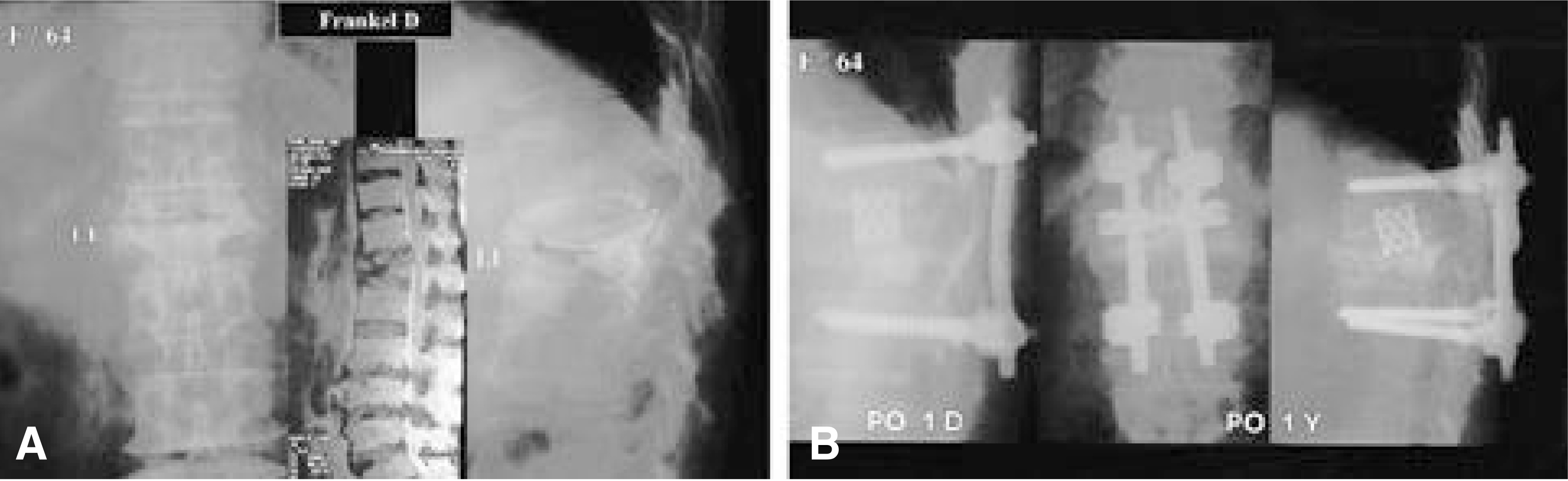
Fig. 4-A. Thoracolumbar spine lateral radiography of a 64-year-old woman shows compression fracture of L1. MRI shows cord compression at L1 level. Fig. 4-B. The cage are inserted due to end plate and intervertebral disc injury during curettage. Collapse is found one year after surgery due to insufficient pedicle screw fixation.
Reference
-
1). Arciero RA, Leung KYT, Pierce JH. Spontaneous unstable burst fracture of the thoracolumbar spine in osteoporosis. Spine. 14:114–117. 1989.
Article2). Brower AC, Downey Jr. and EF Kummel. Diease: Report of a case with serial radiographs. Radiology. 1341:363–364. 1981.3). Hammerberg KW, DeWald RL. Senile burst fracture: a complication of osteoporosis. Orthop Trans. 13:97. 1989.4). Hermann G, Goldblatt J, Desnick RJ. Case reports, Kummell disease: delayed collapse of the traumatized spine in a patient with Gaucher Type 1 disase. The british Journal of Radiology. 57:833–835. 1984.5). Hu SS. Internal fixation in the osteoporotic spine. Spine. 22:s43–s48. 1997.
Article6). Kaneda K, Asano S, Hashimoto T, Satoh S, Fujiya M. The treatment of osteoporotic-posttraumatic vertebral collapse using the Kaneda device and bioactive ceramic vertebral prosthesis. Spine. 17:s295–s303. 1992.7). Kempinsky WH. Osteoporotic kyphosis with paraplegia. Neurology. 8:181–186. 1958.
Article8). Kim SW, Chung YK. The Surgical Reconstruction of Osteoporotic Vertebral Fractures. The Journal of the Korean Society of Fracture. 14:30–36. 2001.
Article9). Lafforgue P, Chagnaud C, Daumen VL, Daver L, Kas-barian M, Acquaviva PC. The intravertebral vacuum phenomenon, migration of intradiscal gas a fractured vertebral body? Spine. 22:1885–1891. 1997.10). Lee CS, Oh WH, Chung SS, et al. Intervertebral Vacu -um Phenomenon. J. of Korean Orthop. Assoc. 33:1148–1156. 1998.11). Maldague BE, Noel HM, malgehm JJ. The intravertebral vacuum cleft. Radilogy. 129:23–29. 1978.12). Parfitt AM, Duncan H. Metabolic bone disease affecting the spine. The Spine. II:second edition. RH Rothman, FA Simone, editors. Philadlphia: WB saunders;p. 828–830. 1982. .).13). Salomon C, Chopin D, Benoist M. Spinal cord compression: An exceptional complication of spinal osteoporosis. Spine. 13:222–224. 1988.14). Shikata J, Yamamuro T, Ida H, Shimizu K, Yoshi kawa J. Surgical treatment for paraplegia resulting from vertebral fractures in senile osteoporosis. Spine. 5:485–489.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterolateral Decompression and Posterior Instrumentation in Lumbar and Thoracolumbar Burst Fracture with Neurologic Deficit
- Surgical Treatment of Osteoporotic Vertebral Fracture with Neurologic Deficits in Thoracolumbar Junction: Comparative Analysis of the Results According to the Surgical Methods
- One-Stage Vertebral Reconstruction Combined with Posterior Instrumentation by Posterolateral Approach for Spinal Metastasis
- Posterolateral Thoracotomy Approach to Tuberculous Spondylitis of the Upper Thoracic Vertebrae
- Treatment of Kümmell’s disease following the occurrence of osteoporotic vertebral compression fracture
