Interobserver Variation in the Diagnosis of Gastric Epithelial Dysplasia and Carcinoma between Two Pathologists in Japan and Korea
- Affiliations
-
- 1Clinical Laboratory Division, National Cancer Center Hospital, Tokyo, Japan.
- 2Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kkmkys@skku.edu
- KMID: 2055510
- DOI: http://doi.org/10.5230/jgc.2011.11.3.141
Abstract
- Although the biological potential of gastric epithelial dysplasia (GED) as a precursor of gastric cancer has never been in doubt, the classification of these lesions has been controversial and fraught with marked variations in approach to diagnosis across the world. The complexity of cyto-architectural features has been considered to be of paramount importance for the diagnosis of carcinoma in Japan, while breach of the basement membrane and invasion into the lamina propria has been considered the sine qua non of malignancy and hence a pre-requisite for the diagnosis of cancer in the West. In Korea, although the incidence of gastric cancer is similar to Japan, the diagnostic approach to GED or cancer seems to lie midway between Western and Japanese criteria. In this review, we will discuss the difference in the diagnosis of GED and cancer between two pathologists working in the comprehensive cancer center located in Japan and Korea, one of the most prevalent areas in the world for gastric cancer.
Keyword
MeSH Terms
Figure
-
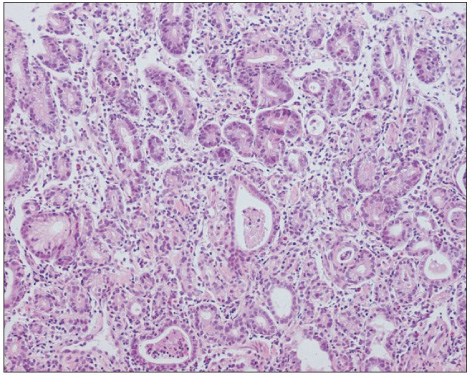
Fig. 1 Gastric biopsies diagnosed as erosion by both RK and KMK. Although the pit shows neutrophilic abscesses, there was no epithelial cell necrosis, suggesting erosion rather than neoplasia.
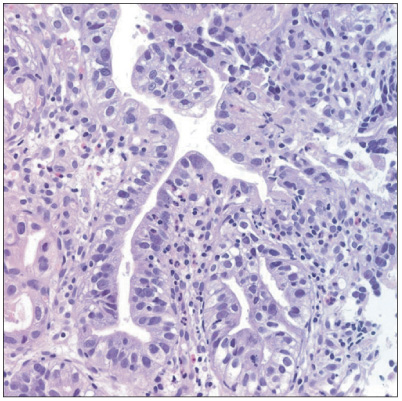
Fig. 2 Gastric biopsies diagnosed as suspected adenocarcinoma by RK. This patient was diagnosed with esophageal squamous cell carcinoma and had received chemo-radiation therapy for 3 months. KMK diagnosed this case as regenerative atypia.
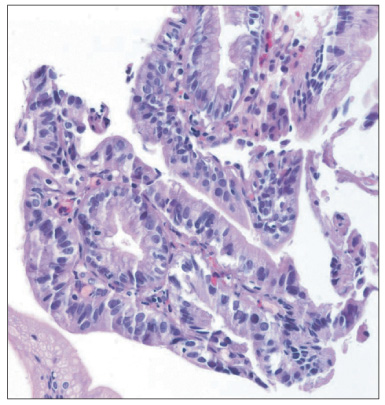
Fig. 3 Gastric biopsies diagnosed as suspicious of adenocarcinoma by KMK. RK diagnosed this case as regenerative atypia because these cells contained Golgi areas in the subapical cytoplasm. KMK thought that those regenerative changes were caused by previous biopsy effects.
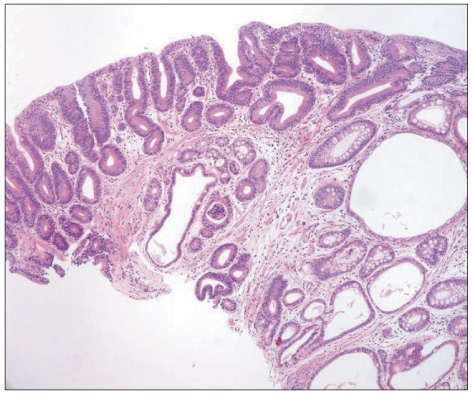
Fig. 4 Gastric biopsies diagnosed as adenoma with low-grade dysplasia by both RK and KMK.

Fig. 5 Representative photomicrograph of a very well differentiated intramucosal intestinal type adenocarcinoma without invasion diagnosed by RK.
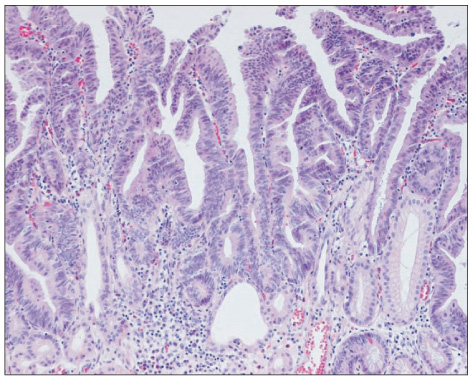
Fig. 6 Representative photomicrograph of an adenocarcinoma diagnosed by RK, but diagnosed as an adenoma with high-grade dysplasia by KMK.

Fig. 7 Representative photomicrograph of gastric type adenocarcinoma diagnosed by RK, but diagnosed as adenoma with high-grade dysplasia by KMK.
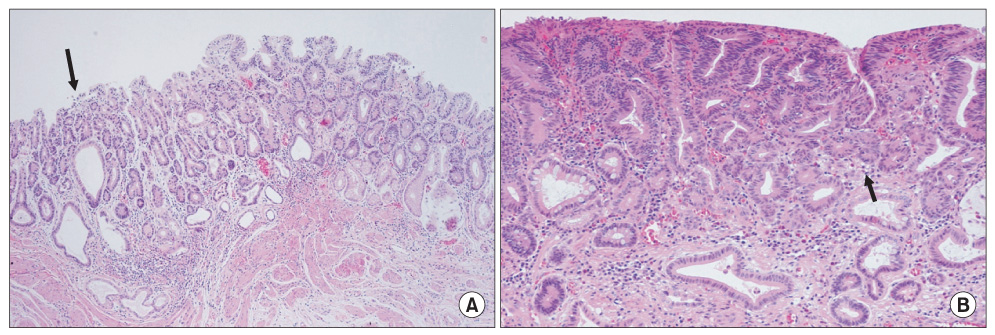
Fig. 8 Adenocarcinoma associated with adenoma diagnosed by RK (A) showing clearly different histology from carcinoma (arrow). Adenocarcinoma arising in adenoma diagnosed by KMK (B) showing a transition from adenoma to carcinoma (arrow).
Cited by 1 articles
-
Inter-observer Reproducibility in the Pathologic Diagnosis of Gastric Intraepithelial Neoplasia and Early Carcinoma in Endoscopic Submucosal Dissection Specimens: A Multi-center Study
Joon Mee Kim, Jin Hee Sohn, Mee-Yon Cho, Woo Ho Kim, Hee Kyung Chang, Eun Sun Jung, Myeong-Cherl Kook, So-Young Jin, Yang Seok Chae, Young Soo Park, Mi Seon Kang, Hyunki Kim, Jae Hyuk Lee, Do Youn Park, Kyoung Mee Kim, Hoguen Kim, Young Ju Suh, Sang Yong Seol, Hwoon-Yong Jung, Deuck–Hwa Kim, Na Rae Lee, Seung-Hee Park, Ji Hye You
Cancer Res Treat. 2019;51(4):1568-1577. doi: 10.4143/crt.2019.019.
Reference
-
1. Rugge M, Correa P, Dixon MF, Hattori T, Leandro G, Lewin K, et al. Gastric dysplasia: the Padova international classification. Am J Surg Pathol. 2000. 24:167–176.2. Montgomery E, Bronner MP, Goldblum JR, Greenson JK, Haber MM, Hart J, et al. Reproducibility of the diagnosis of dysplasia in Barrett esophagus: a reaffirmation. Hum Pathol. 2001. 32:368–378.
Article3. Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO Classification of Tumours of the Digestive System. 2010. 4th ed. Lyon: World Health Organization;10–14.4. Downs-Kelly E, Mendelin JE, Bennett AE, Castilla E, Henricks WH, Schoenfield L, et al. Poor interobserver agreement in the distinction of high-grade dysplasia and adenocarcinoma in pretreatment Barrett's esophagus biopsies. Am J Gastroenterol. 2008. 103:2333–2340.
Article5. Schlemper RJ, Itabashi M, Kato Y, Lewin KJ, Riddell RH, Shimoda T, et al. Differences in diagnostic criteria for gastric carcinoma between Japanese and western pathologists. Lancet. 1997. 349:1725–1729.
Article6. Kim JM, Cho MY, Sohn JH, Kang DY, Park CK, Kim WH, et al. Gastrointestinal Pathology Study Group of Korean Society of Pathologists. Diagnosis of gastric epithelial neoplasia: Dilemma for Korean pathologists. World J Gastroenterol. 2011. 17:2602–2610.
Article7. Schlemper RJ, Riddell RH, Kato Y, Borchard F, Cooper HS, Dawsey SM, et al. The Vienna classification of gastrointestinal epithelial neoplasia. Gut. 2000. 47:251–255.
Article8. Stolte M. The new Vienna classification of epithelial neoplasia of the gastrointestinal tract: advantages and disadvantages. Virchows Arch. 2003. 442:99–106.
Article9. Kim WH, Park CK, Kim YB, Kim YW, Kim HG, Bae HI, et al. A standardized pathology report for gastric cancer. Korean J Pathol. 2005. 39:106–113.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pathologic Diagnosis of Gastric Epithelial Neoplasia
- Interobserver diagnostic reproducibility in advanced-stage endometrial carcinoma
- Interobserver Variability and Accuracy of High-Definition Endoscopic Diagnosis for Gastric Intestinal Metaplasia among Experienced and Inexperienced Endoscopists
- Interobserver Variability in Diagnosing High-Grade Neuroendocrine Carcinoma of the Lung and Comparing It with the Morphometric Analysis
- Expression of Carbohydrate Antigens in Gastric Epithelial Dysplasia and Gastric Carcinoma by Immunohistochemistry
