Pre-operative Evaluation of Eustachian Tube Function Using a Modified Pressure Equilibration Test is Predictive of Good Postoperative Hearing and Middle Ear Aeration in Type 1 Tympanoplasty Patients
- Affiliations
-
- 1Department of Otolaryngology, Jeju National University Hospital, Jeju National University, College of Medicine, Jeju, Korea.
- 2Department of Otolaryngology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jwchung@amc.seoul.kr
- KMID: 2007186
- DOI: http://doi.org/10.3342/ceo.2009.2.2.61
Abstract
OBJECTIVES
The Eustachian tube (ET) plays an important role in maintaining a normally aerated middle ear. Inflammation in middle ear disease is related to ET dysfunction, and postoperative restoration of middle ear integrity and hearing are closely related to ET function in chronic ear disease patients. After successful tympanoplasty, restoration of a well-aerated middle ear with good ET function can permit better compliance of the tympanic membrane. In this study, we evaluated the predictive validity of preoperative ET function measurements.
METHODS
We reviewed 137 patients who underwent type 1 tympanoplasty. All patients had non-cholesteatomatous chronic otitis media and received canal wall-up-type tympanomastoidectomies. Patients were categorized into four groups according to preoperative ET function measurements using a modified pressure inflation-deflation equilibration test. Group I patients had residual pressures less than 10 daPa, and Group IV patients showed no pressure change (poor results). Groups II and III were intermediate. Hearing levels were determined using pure tone averages at four frequencies. Postoperative tympanography was performed to determine middle ear aeration.
RESULTS
The preoperative air bone (AB) gap was 29.6+/-7.0 dB, and the postoperative gap was 16.5+/-5.7 dB; thus, there was significant overall improvement. In all groups, hearing was significantly better after surgery, but the worst postoperative hearing level was seen in Group IV patients. Type B tympanograms were more frequently recorded in Group IV patients than they were in Group I or II patients. Postoperative AB gaps were 9.2+/-3.8 dB in patients with type A tympanograms, 13.4+/-2.1 dB in those with type As, 24.1+/-2.5 dB in those with type C, and 18.5+/-2.8 dB in those with type B.
CONCLUSION
ET function measured with a modified pressure equilibration test using an inflation-deflation manometric method is a good indicator of an aerated middle ear and is predictive of improved postoperative hearing.
Keyword
MeSH Terms
Figure
-

Fig. 1 Examples of recordings from the pressure equilibration test, showing residual pressure (Pr). Group I ears completely equilibrated to both positive and negative pressures (Pr<10 daPa and >-10 daPa, respectively). Group II ears partially equilibrated to both positive and negative pressures (Pr>10 daPa and <-10 daPa, respectively). Group III ears completely or partially equilibrated to positive pressure, but could not equilibrate to negative pressure. Group IV ears could not equilibrate to either positive or negative pressure.
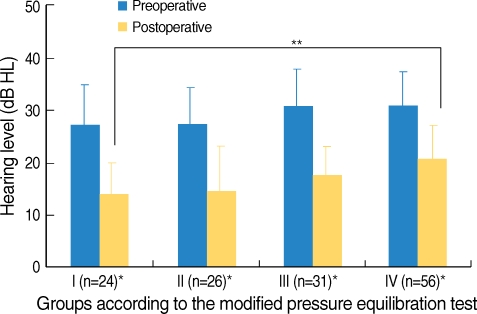
Fig. 2 Mean preoperative and postoperative hearing levels of groups classified with respect to results of the modified pressure equilibration test.*Postoperative hearing was better than preoperative hearing was in all groups (P<0.05). **The postoperative hearing of Group IV patients was significantly worse than that of Group I patients (P<0.01).
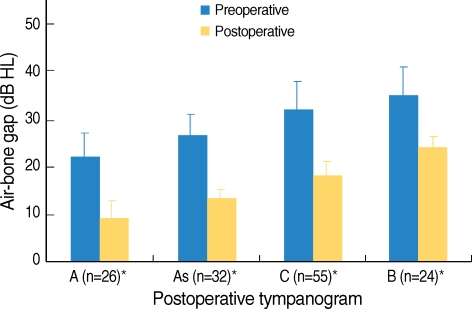
Fig. 3 Preoperative and postoperative hearing levels of patients classified into different types with respect to postoperative tympanography.*Postoperative hearing was better than preoperative hearing was in all patient types (P<0.05).
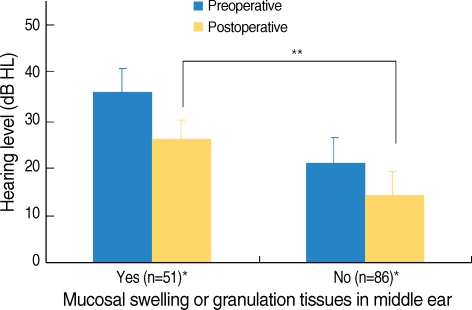
Fig. 4 Preoperative and postoperative hearing levels of patients with or without middle ear mucosal swelling and granulation tissue.*Postoperative hearing was better than preoperative hearing was in both groups (P<0.05). **The postoperative hearing level of patients with mucosal swelling and granulation tissue was significantly worse than that of patients without such complications (P<0.01).
Reference
-
1. Lin AC, Messner AH. Pediatric tympanoplasty: factors affecting success. Curr Opin Otolaryngol Head Neck Surg. 2008; 2. 16(1):64–68. PMID: 18197025.
Article2. Bellucci RJ. Selection of cases and classification of tympanoplasty. Otolaryngol Clin North Am. 1989; 10. 22(5):911–926. PMID: 2694069.3. Vartiainen E, Nuutinen J. Success and pitfalls in myringoplasty: follow-up study of 404 cases. Am J Otol. 1993; 5. 14(3):301–305. PMID: 8372930.4. Todd NW. There are no accurate tests for eustachian tube function. Arch Otolaryngol Head Neck Surg. 2000; 8. 126(8):1041–1042. PMID: 10922245.
Article5. Takahashi H, Sato H, Nakamura H, Naito Y, Umeki H. Correlation between middle-ear pressure-regulation functions and outcome of type-I tympanoplasty. Auris Nasus Larynx. 2007; 6. 34(2):173–176. PMID: 17055205.
Article6. Uzun C. Cartilage palisade tympanoplasty, diving and eustachian tube function. Otol Neurotol. 2003; 3. 24(2):350. PMID: 12621358.
Article7. Jerger J. Clinical experience with impedance audiometry. Arch Otolaryngol. 1970; 10. 92(4):311–324. PMID: 5455571.
Article8. Yuceturk AV, Unlu HH, Okumus M, Yildiz T, Filiz U. The evaluation of eustachian tube function in patients with chronic otitis media. Clin Otolaryngol Allied Sci. 1997; 10. 22(5):449–452. PMID: 9372257.
Article9. Straetemans M, van Heerbeek N, Schilder AG, Feuth T, Rijkers GT, Zielhuis GA. Eustachian tube function before recurrence of otitis media with effusion. Arch Otolaryngol Head Neck Surg. 2005; 2. 131(2):118–123. PMID: 15723942.
Article10. van Heerbeek N, Ingels KJ, Snik AF, Zielhuis GA. Eustachian tube function in children after insertion of ventilation tubes. Ann Otol Rhinol Laryngol. 2001; 12. 110(12):1141–1146. PMID: 11768705.
Article11. American Academy of Otolaryngology-Head and Neck Surgery Foundation, Inc. Committee on Hearing and Equilibrium guidelines for the evaluation of results of treatment of conductive hearing loss. Otolaryngol Head Neck Surg. 1995; 9. 113(3):186–187. PMID: 7675477.12. Fowler CG, Shanks JE. Katz J, Burkard RF, Medwetsky L, editors. Tympanometry. Handbook of clinical audiology. 2002. 5th ed. Philadelphia (PA): Lippincott Williams & Wilkins;p. 175–204.13. Ikarashi F, Tsuchiya A. Middle ear gas exchange via the mucosa: estimation by hyperventilation. Acta Otolaryngol. 2008; 1. 128(1):9–12. PMID: 18158641.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Eustachian Tube Function and Mastoid Pneumatization as Prognostic Factors of Type 1 Tympanoplasty
- Change of Tympanogram after Chronic Otitis Media Surgery
- The Value of Measuring Eustachian Tube Aeration on Temporal Bone CT in Patients with Chronic Otitis Media
- Hearing Results After Type I Tympanoplasty With Versus Without Mastoidectomy
- Cartilage-Perichondrium Tympanoplasty for Pediatric Atelectatic Ears
