Positioning During CT Gastrography in Patients with Gastric Cancer: the Effect on Gastric Distension and Lesion Conspicuity
- Affiliations
-
- 1Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul 138-736, Korea. aykim@amc.seoul.kr
- 2Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul 138-736, Korea.
- 3Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul 138-736, Korea.
- 4Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul 138-736, Korea.
- KMID: 1779452
- DOI: http://doi.org/10.3348/kjr.2009.10.3.252
Abstract
OBJECTIVE
We wanted to prospectively evaluate the effect of various positions of the patient on gastric distension and lesion conspicuity during performance of CT gastrography (CTG). MATERIALS AND METHODS: One hundred thirteen consecutive patients with gastric cancer underwent CTG in the 30degrees left posterior oblique (LPO), supine, and prone positions. Two radiologists scored (a grade from 1-4) the degree of gastric distension and the lesion conspicuity according to the three scanning positions and the three gastric portions. Two- (2D) and three-dimensional (3D) images were used for analysis. Finally, these data were compared with the endoscopic findings and surgical results. RESULTS: The mean scores of gastric distension and lesion conspicuity for the LPO and supine positions were higher than those for the prone position (p < 0.001) in the gastric middle and lower portions. However, there was no significant difference between the LPO and supine positions (p > or = 0.21). As for the gastric upper portion, the mean scores of gastric distension in the prone position were higher than those in the two other positions (p < 0.001). The prone position showed better lesion conspicuity than the two other positions for only one of two cases of gastric cancer in the upper portion of the stomach. CONCLUSION: CTG performed in the LPO position or the supine position combined with CTG performed in the prone position is optimal for achieving good gastric distension and evaluating the lesion conspicuity of gastric cancer.
MeSH Terms
Figure
-

Fig. 1 51-year-old woman who underwent CT gastrography according to three scanning positions. On two-dimensional axial images, grade of distension of gastric lower portion was 4 (more than 75%) in 30° left posterior oblique position (A), 3 (between 50% and 75% of expected maximal distension) in supine position (B), and 3 in prone position (C). As for gastric upper portion, grade of distension was 3 in 30° left posterior oblique position (D), 3 in supine position (E), and 4 in prone position (F).
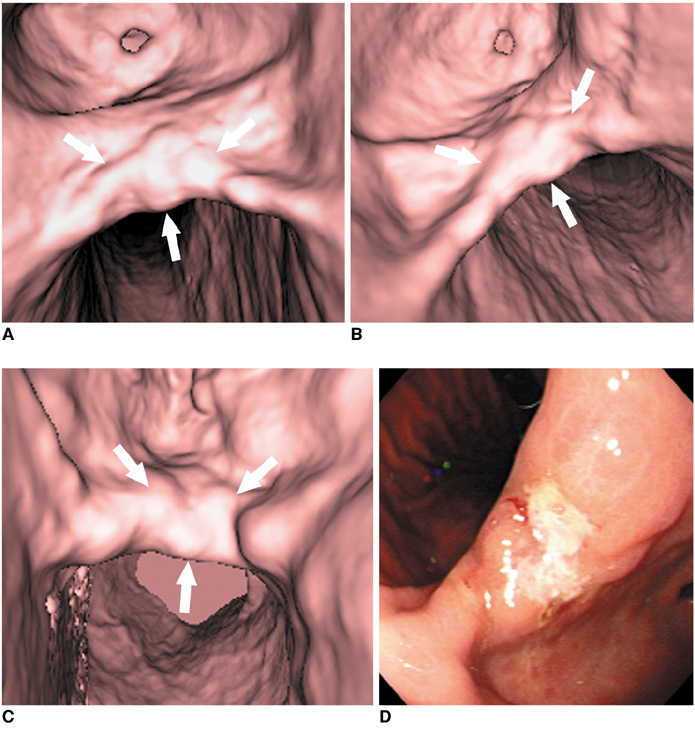
Fig. 2 65-year-old man with early gastric cancer in middle portion. This lesion shows irregular mucosal nodularity with depressed lesion in gastric angle (arrows in A-C). Grade of lesion conspicuity in both 30° left posterior oblique (A) and supine positions (B) was 4 (good). However, lesion conspicuity in prone position (C) was 2 (poor) due to partially collapsed stomach with exaggerated rugal folds. This fiberoptic gastroscopic finding well corresponds to virtual gastroscopic images (D). This lesion was histopathologically diagnosed as early gastric cancer after surgery.

Fig. 3 53-year-old man with advanced gastric cancer in upper portion. This lesion shows ulcerofungating mass in upper portion (arrows in B, C). Lesion conspicuity in 30° left posterior oblique position (A) was 1 (not detectable) due to retained fluid, whereas grade of lesion conspicuity in both supine (B) and prone positions (C) was 4 (good). Fiberoptic gastroscopic findings (D) and surgical specimen (E) well corresponds to surface shaded display images. This lesion was histopathologically diagnosed as advanced gastric cancer.
Cited by 1 articles
-
The Role of Three-Dimensional Multidetector CT Gastrography in the Preoperative Imaging of Stomach Cancer: Emphasis on Detection and Localization of the Tumor
Jin Woong Kim, Sang Soo Shin, Suk Hee Heo, Hyo Soon Lim, Nam Yeol Lim, Young Kyu Park, Yong Yeon Jeong, Heoung Keun Kang
Korean J Radiol. 2015;16(1):80-89. doi: 10.3348/kjr.2015.16.1.80.
Reference
-
1. Forman D, Goodman KJ. The epidemiology of stomach cancer: correlating the past with the present. Socioeconomic influences in early life can influence mortality in adult life. BMJ. 2000. 320:1682–1683.2. Houghton J, Wang TC. Feldman , editor. Tumors of the stomach. Sleisenger and Fordtran's gastrointestinal and liver disease. 2006. 8th eds. Philadelphia: Saunders;1139–1156.3. Habermann CR, Weiss F, Riecken R, Honarpisheh H, Bohnacker S, Staedtler C, et al. Preoperative staging of gastric adenocarcinoma: comparison of helical CT and endoscopic US. Radiology. 2004. 230:465–471.4. Kim AY, Kim HJ, Ha HK. Gastric cancer by multidetector row CT: preoperative staging. Abdom Imaging. 2005. 30:465–472.5. Kim HJ, Kim AY, Oh ST, Kim JS, Kim KW, Kim PN, et al. Gastric cancer staging at multi-detector row CT gastrography: comparison of transverse and volumetric CT scanning. Radiology. 2005. 236:879–885.6. Kim JH, Park SH, Hong HS, Auh YH. CT gastrography. Abdom Imaging. 2005. 30:509–517.7. Kumano S, Murakami T, Kim T, Hori M, Iannaccone R, Nakata S, et al. T staging of gastric cancer: role of multi-detector row CT. Radiology. 2005. 237:961–966.8. Chen CY, Hsu JS, Wu DC, Kang WY, Hsieh JS, Jaw TS, et al. Gastric cancer: preoperative local staging with 3D multidetector row CT-correlation with surgical and histopathologic results. Radiology. 2007. 242:472–482.9. Springer P, Dessl A, Giacomuzzi SM, Buchberger W, Stöger A, Oberwalder M, et al. Virtual computed tomography gastroscopy: a new technique. Endoscopy. 1997. 29:632–634.10. Ogata I, Komohara Y, Yamashita Y, Mitsuzaki K, Takahashi M, Ogawa M. CT evaluation of gastric lesions with three-dimensional display and interactive virtual endoscopy: comparison with conventional barium study and endoscopy. AJR Am J Roentgenol. 1999. 172:1263–1270.11. Kim H, Takashima S, Kaminou T, Hayashi S, Nishida N, Matsuoka T, et al. Clinical studies on the visualization of gastric lesions using virtual CT endoscopy. Osaka City Med J. 2001. 47:115–126.12. Oto A. Virtual endoscopy. Eur J Radiol. 2002. 42:231–239.13. Kim SH, Han JK, Lee KH, Chung JW, Yang HK, Choi BI. Computed tomography gastrography with volume-rendering technique: correlation with double-contrast barium study and conventional gastroscopy. J Comput Assist Tomogr. 2003. 27:140–149.14. Bhandari S, Shim CS, Kim JH, Jung IS, Cho JY, Lee JS, et al. Usefulness of three-dimensional, multidetector row CT (virtual gastroscopy and multiplanar reconstruction) in the evaluation of gastric cancer: a comparison with conventional endoscopy, EUS, and histopathology. Gastrointest Endosc. 2004. 59:619–626.15. Inamoto K, Kouzai K, Ueeda T, Marukawa T. CT virtual endoscopy of the stomach: comparison study with gastric fiberscopy. Abdom Imaging. 2005. 30:473–479.16. Carrascosa P, Capuńay C, Ulla M, López EM, Corti R, Carrascosa J. Elevated gastric lesions: virtual gastroscopy. Abdom Imaging. 2006. 31:261–267.17. Kim JH, Eun HW, Hong SS, Auh YH. Early gastric cancer: virtual gastroscopy. Abdom Imaging. 2006. 31:507–513.18. Lee DH, Ko YT. Gastric lesions: evaluation with three-dimensional images using helical CT. AJR Am J Roentgenol. 1997. 169:787–789.19. Lee DH, Ko YT. The role of 3D spiral CT in early gastric carcinoma. J Comput Assist Tomogr. 1998. 22:709–713.20. Lee DH, Ko YT. Advanced gastric carcinoma: the role of three-dimensional and axial imaging by spiral CT. Abdom Imaging. 1999. 24:111–116.21. Kim SH, Lee JM, Han JK, Lee JY, Yang HK, Lee HJ, et al. Effect of adjusted positioning on gastric distention and fluid distribution during CT gastrography. AJR Am J Roentgenol. 2005. 185:1180–1184.22. Oda I, Saito D, Tada M, Iishi H, Tanabe S, Oyama T, et al. A multicenter retrospective study of endoscopic resection for early gastric cancer. Gastric Cancer. 2006. 9:262–270.23. Kim JH, Eun HW, Choi JH, Hong SS, Kang W, Auh YH. Diagnostic performance of virtual gastroscopy using MDCT in early gastric cancer compared with 2D axial CT: focusing on interobserver variation. AJR Am J Roentgenol. 2007. 189:299–305.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefullness of CT Gastrography and Vurtual Gastroscopy using Computed Tomography in Detection of Gastric Cancer
- Usefulness of Computed Tomography Gastrography in the Surgical Management of a Gastric GIST
- Measurement of the Mucosal Surface Distance in the Early Gastric Cancer Using CT Gastrography
- The Role of Three-Dimensional Multidetector CT Gastrography in the Preoperative Imaging of Stomach Cancer: Emphasis on Detection and Localization of the Tumor
- Diagnostic significance of gas distension technique of the stomach with gas-forming agent on CT scan of stomach cancer
