Congenital Stapes Anomalies with Normal Eardrum
- Affiliations
-
- 1Department of Otolaryngology, Ajou University School of Medicine, Suwon, Korea. parkkh@ajou.ac.kr
- KMID: 1466561
- DOI: http://doi.org/10.3342/ceo.2009.2.1.33
Abstract
OBJECTIVES
A non-progressive and conductive hearing loss with normal eardrum, but no history of trauma and infection, is highly suggestive of a congenital ossicular malformation. Among ossicular anomalies, stapes anomaly is the most common. The purpose of this study is to describe patterns of stapes anomaly and to analyze its surgical outcome with special reference to its patterns.
METHODS
We conducted a retrospective case review. The subjects comprised 66 patients (76 ears) who were decisively confirmed by the exploratory tympanotomy as congenital stapes anomalies without any anomalies of the tympanic membrane and external auditory canal. The preoperative and postoperative audiological findings, temporal bone computed tomography scan, and operative findings were analyzed.
RESULTS
There were 16 anomalous patterns of stapes among which footplate fixation was the most common anomaly. These 16 patterns were classified into 4 types according to the status of stapes footplate. Successful hearing gain was achieved in 51 out of 76 ears (67.1%) after surgical treatment.
CONCLUSION
Footplate fixation was usually bilateral, whereas stapes anomalies associated with other ossicular anomaly were usually unilateral. The success of the surgical treatment of stapes anomaly might depend on its developmental status of the footplate. Stapes anomalies were detected without any fixed patterns, therefore, it is quite possible to detect a large variety of patterns in future.
MeSH Terms
Figure
-
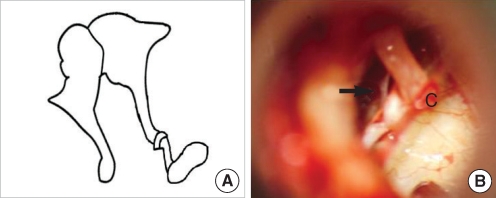
Fig. 1 Stapes without anterior crus. (A) Schematic presentation. (B) Operative finding shows no anterior crus of the stapes (arrow).c: chorda tympani.
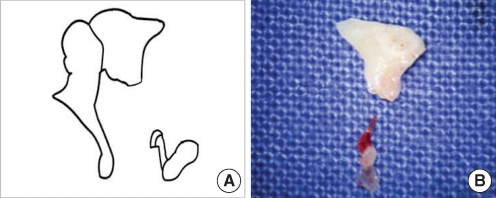
Fig. 2 Stapes without anterior crus and incus long process. (A) Schematic presentation. (B) Removed incus shows no long process, and removed stapes shows no anterior crus.
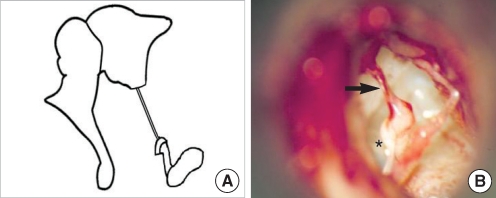
Fig. 3 Stapes without anterior crus and incus long process with fibrous band. (A) Schematic presentation. (B) Operative finding shows a fibrous band (arrow) instead of the incus long process and the stapes lacking anterior crus (asterisk).
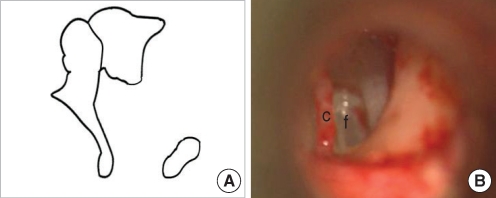
Fig. 4 Stapes without superstructure and incus long process. (A) Schematic presentation. (B) Operative finding shows no incus long process and no stapes superstructure.c: chorda tympani; f: footplate.
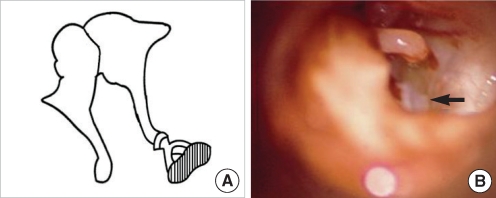
Fig. 5 Stapes footplate fixation. (A) Schematic presentation. (B) Operative finding shows half of the stapes footplate remaining (arrow) because of partial fixation of its footplate.
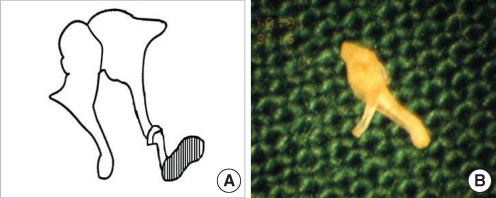
Fig. 6 Stapes footplate fixation without anterior crus. (A) Schematic presentation. (B) Removed stapes shows an underdeveloped anterior crus.
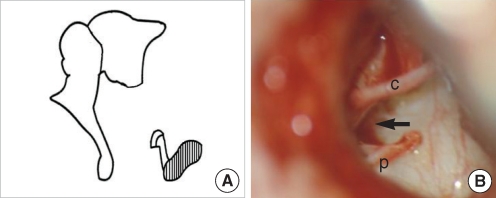
Fig. 7 Stapes footplate fixation without anterior crus and incus long process. (A) Schematic presentation. (B) Operative finding shows no incus long process and the stapes lacking anterior crus (arrow) without mobility of its footplate. c: chorda tympani; p: posterior crus.
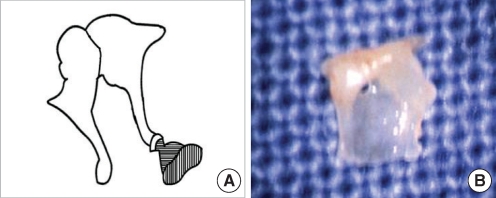
Fig. 8 Stapes footplate fixation with obturator foramen obliteration. (A) Schematic presentation. (B) Removed stapes shows a non-perforated obturator foramen.
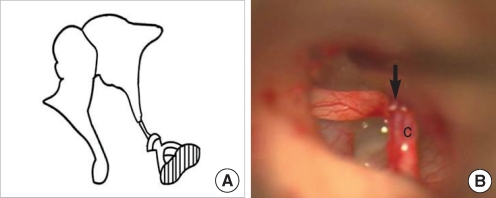
Fig. 9 Stapes footplate fixation without lenticular process: only fibrous band. (A) Schematic presentation. (B) Operative finding shows a fibrous band (arrow) instead of the lenticular process of the incus.c: chorda tympani.
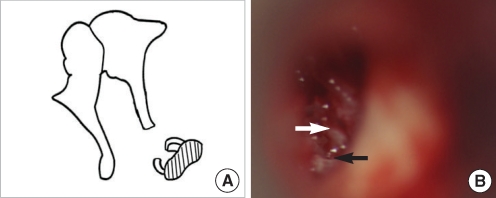
Fig. 10 Stapes footplate fixation without stapes head. (A) Schematic presentation. (B) Operative finding shows only anterior (white arrow) and posterior crus (black arrow) without mobility of its footplate.
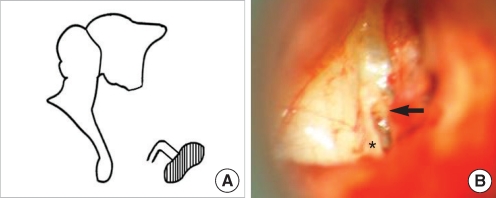
Fig. 11 Stapes footplate fixation with monopolar crus and without incus long process. (A) Schematic presentation. (B) Operative finding shows only one crus in the center of the footplate (arrow) and stapes-pyramidal fixation by a bony bar (asterisk).
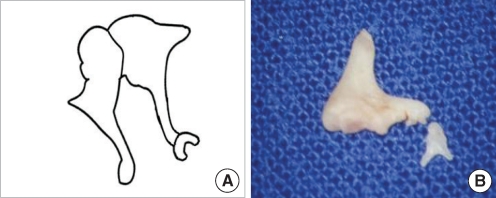
Fig. 12 Underdeveloped stapes crura without oval window. (A) Schematic presentation. (B) Removed stapes shows underdeveloped crura.
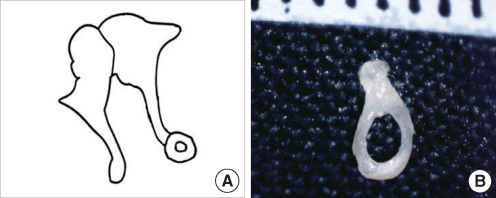
Fig. 13 Anterior and posterior crura fusion without oval window. (A) Schematic presentation. (B) Removed stapes shows a crural fusion.
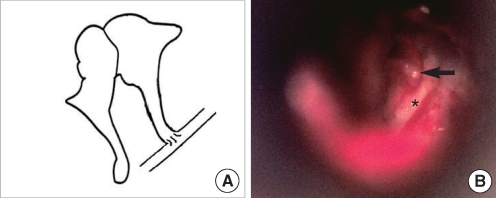
Fig. 14 No stapes and no oval window. (A) Schematic presentation. (B) Operative finding shows a long process of the incus (arrow) without the stapes, which is in contact with a downward facial nerve (asterisk) in the mesotympanum.
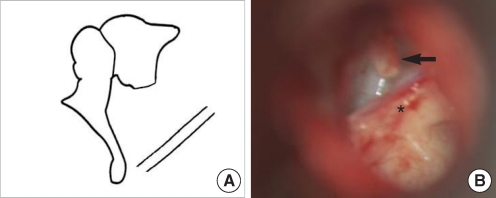
Fig. 15 No stapes and no oval window without incus long process. (A) Schematic presentation. (B) Operative finding shows shortening of the incus long process (arrow) without the stapes and downward displacement of the tympanic portion of the facial nerve with a bony bar (asterisk).
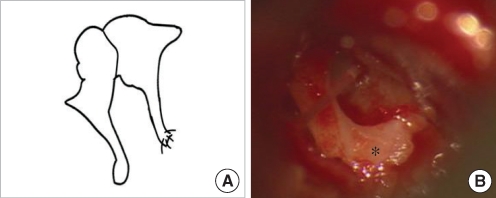
Fig. 16 No stapes and no oval window with incus long process fused to promontorium. (A) Schematic presentation. (B) Operative finding shows the long process of the incus fused to promontorium (asterisk) without the stapes and the oval window.
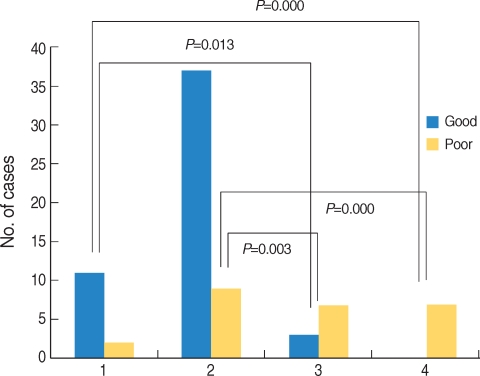
Fig. 17 Comparison of postoperative hearing results of congenital stapes anomaly according to status of stapes footplate (76 ears). Patients with mobile stapes or only stapes footplate fixation had significantly better hearing result than patients with stapes fixation associated with other ossicular anomaly or no stapes footplate.1: Mobile stapes footplate with other anomaly; 2: Stapes footplate fixation only; 3: Stapes footplate fixation with other anomaly; 4: No stapes footplate with other anomaly; Good: postoperative air-bone gap <20 dB; Poor: postoperative air-bone gap ≥20 dB. Postoperative air-bone gap: postoperative air conduction-preoperative bone conduction.
Reference
-
1. House HP, House WF, Hildyard VH. Congenital stapes footplate fixation: a preliminary report of twenty-three operated cases. Laryngoscope. 1958; 8. 68(8):1389–1402. PMID: 13576898.
Article2. Lindsay JR, Sanders SH, Nager GT. Histopathologic observations in so-called congenital fixation of the stapedial footplate. Laryngoscope. 1960; 12. 70(12):1587–1602. PMID: 13762396.
Article3. Gundersen T. Congenital malformations of the stapes footplate. Arch Otolaryngol. 1967; 2. 85(2):171–176. PMID: 6017589.
Article4. Steele BC. Congenital fixation of the stapes footplate. Acta Otolaryngol. 1969; (Suppl 245):1–24. PMID: 5379836.5. Teunissen B, Cremers WR, Huygen PL, Pouwels TP. Isolated congenital stapes ankylosis: surgical results in 32 ears and a review of the literature. Laryngoscope. 1990; 12. 100(12):1331–1336. PMID: 2243529.6. Nandapalan V, Tos M. Isolated congenital stapes ankylosis: an embryologic survey and literature review. Am J Otol. 2000; 1. 21(1):71–80. PMID: 10651438.
Article7. Albert S, Roger G, Rouillon I, Chauvin P, Denoyelle F, Derbez R, et al. Congenital stapes ankylosis: study of 28 cases and surgical results. Laryngoscope. 2006; 7. 116(7):1153–1157. PMID: 16826051.
Article8. Schlosser WD, Goldman BR, Winchester RA. Further experiences with the diagnosis and surgical management of congenital mixed deafness. Laryngoscope. 1964; 6. 74:773–789. PMID: 14171385.
Article9. Hashimoto S, Yamamoto Y, Satoh H, Takahashi S. Surgical treatment of 52 cases of auditory ossicular malformations. Auris Nasus Larynx. 2002; 1. 29(1):15–18. PMID: 11772485.
Article10. Committee on Hearing and Equilibrium. Committee on hearing and equilibrium guidelines for the evaluation of results of treatment of conductive hearing loss. Otolaryngol Head Neck Surg. 1995; 9. 113(3):186–187. PMID: 7675477.11. Dass R, Grewal BS, Thapar SP. Human stapes and its variations. II. Footplate. J Laryngol Otol. 1966; 5. 80(5):471–480. PMID: 5934111.12. Yuen HY, Ahuja AT, Wong KT, Yue V, van Hasselt AC. Computed tomography of common congenital lesions of the temporal bone. Clin Radiol. 2003; 9. 58(9):687–693. PMID: 12943639.
Article13. Raveh E, Hu W, Papsin BC, Forte V. Congenital conductive hearing loss. J Laryngol Otol. 2002; 2. 116(2):92–96. PMID: 11827579.
Article14. Hung KL, Tu TY, Tsai TL, Shiao AS. Congenital ossicular anomalies. J Chin Med Assoc. 2003; 8. 66(8):474–479. PMID: 14604311.15. Dornhoffer JL, Helms J, Hoehmann DH. Stapedectomy for congenital fixation of the stapes. Am J Otol. 1995; 5. 16(3):382–386. PMID: 8588635.16. Cremers CW, Hoogland GA. Congenital stapes ankylosis by elongation of the pyramidal eminence. Ann Otol Rhinol Laryngol. 1986; Mar–Apr. 95(2 Pt 1):167–168. PMID: 3963687.17. Teunissen B, Cremers CW. Surgery for congenital stapes ankylosis with an associated congenital ossicular chain anomaly. Int J Pediatr Otorhinolaryngol. 1991; 5. 21(3):217–226. PMID: 1869375.
Article18. Kinsella JB, Kerr AG. Familial stapes superstructure fixation. J Laryngol Otol. 1993; 1. 107(1):36–38. PMID: 8445310.
Article19. Nandapalan V, Tos M. Isolated congenital stapes suprastructure fixation. J Laryngol Otol. 1999; 9. 113(9):798–802. PMID: 10664680.
Article
