Carney Complex in Three First-Degree Relatives
- Affiliations
-
- 1Department of Radiology, Eulji University Hospital, Korea. kskim@eulji.ac.kr
- KMID: 1460076
- DOI: http://doi.org/10.3348/jksr.2010.62.4.393
Abstract
- The Carney complex, the first reported in a series of 40 patients by J. A. Carney in 1985, is an autosomal dominant disease that is characterized by multiple neoplasia. The disease has a familial pattern in approximately one-half of the patients. We present the three cases of the Carney complex within one family.
Figure
-
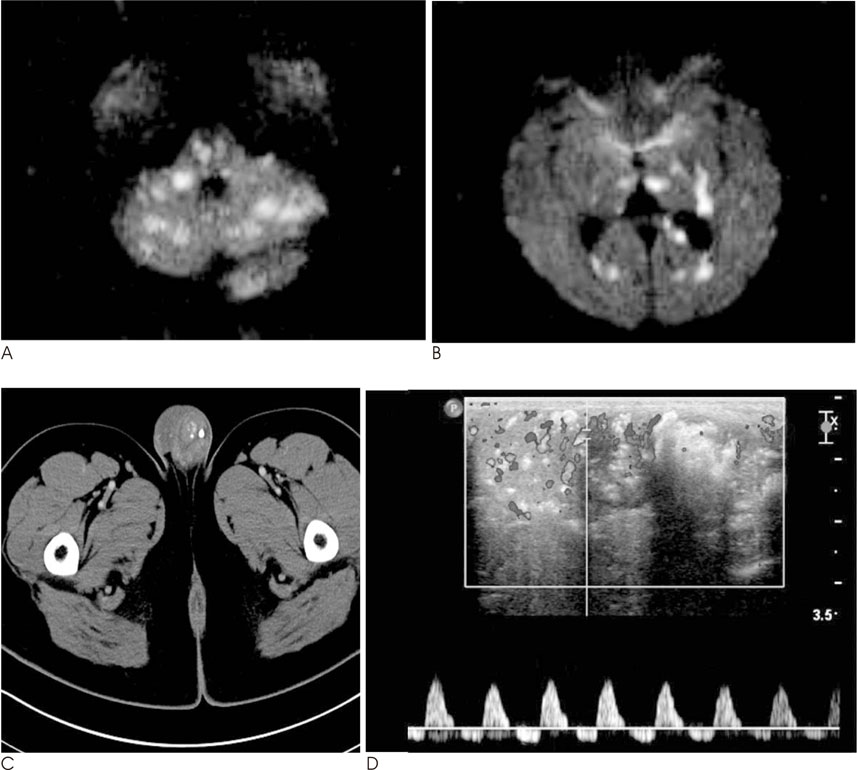
Fig. 1 Case 1. A, B. Cerebral infarction due to a cardiogenic embolism (case 1). Diffusion weighted MR images show multiple high signal intensities involving the cerebellar hemispheres, pons, midbrain, thalami, left hippocampus, the body and splenium of the corpus callosum, both cerebral cortices, and subcortical white matter. These findings are typical of a cardiogenic embolic infarction. C. A Pelvic CT scan shows the asymmetric enlargement and internal calcification in the left testis. D. A scrotal sonography shows complex masses with irregular calcification patterns and heavy posterior acoustic shadowing. Increased arterial flow around the nodules is also noted.
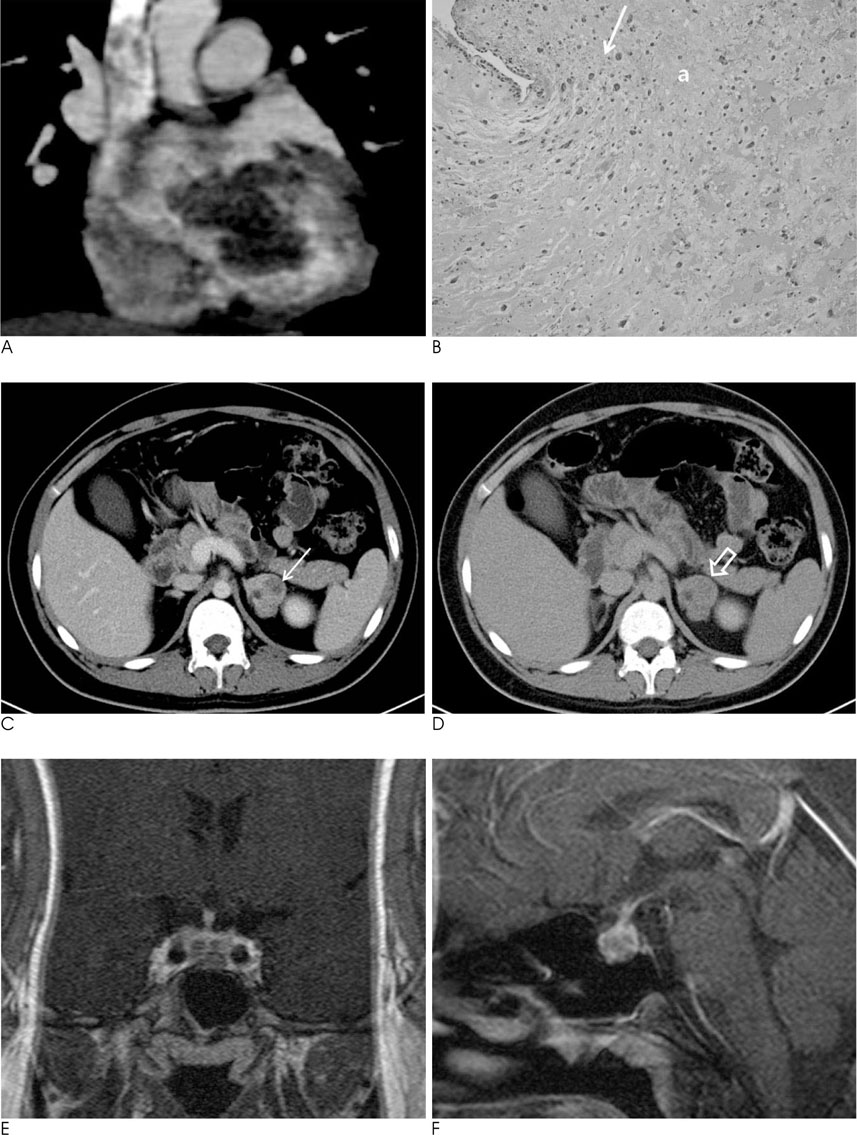
Fig. 2 Case 2. A. Coronal reformatted CT images with contrast enhancement show the lobular mass (5 × 4 × 6 cm) with mild contrast enhancement in the left atrium. B. Cardiac myxoma shows tumor cells (arrow) concentrated just beneath the surface, and surrounded by an abundant myxoid stroma (a) (hematoxylin and eosin stain, original magnification × 1.0). C. Arterial CT image shows a large mass (arrow, 3.5 cm in maximum diameter) with strong enhancement in the left adrenal gland. D. An axial CT scan after 10 minutes shows the delayed wash-out of the contrast agent in the nodule (open arrow). The absolute wash-out percentage was calculated to be 63%. E, F. Coronal (E) and sagittal (F) MR images with gadolinum-enhancement show an enlargement of the pituitary gland with multiple enhancing nodules.
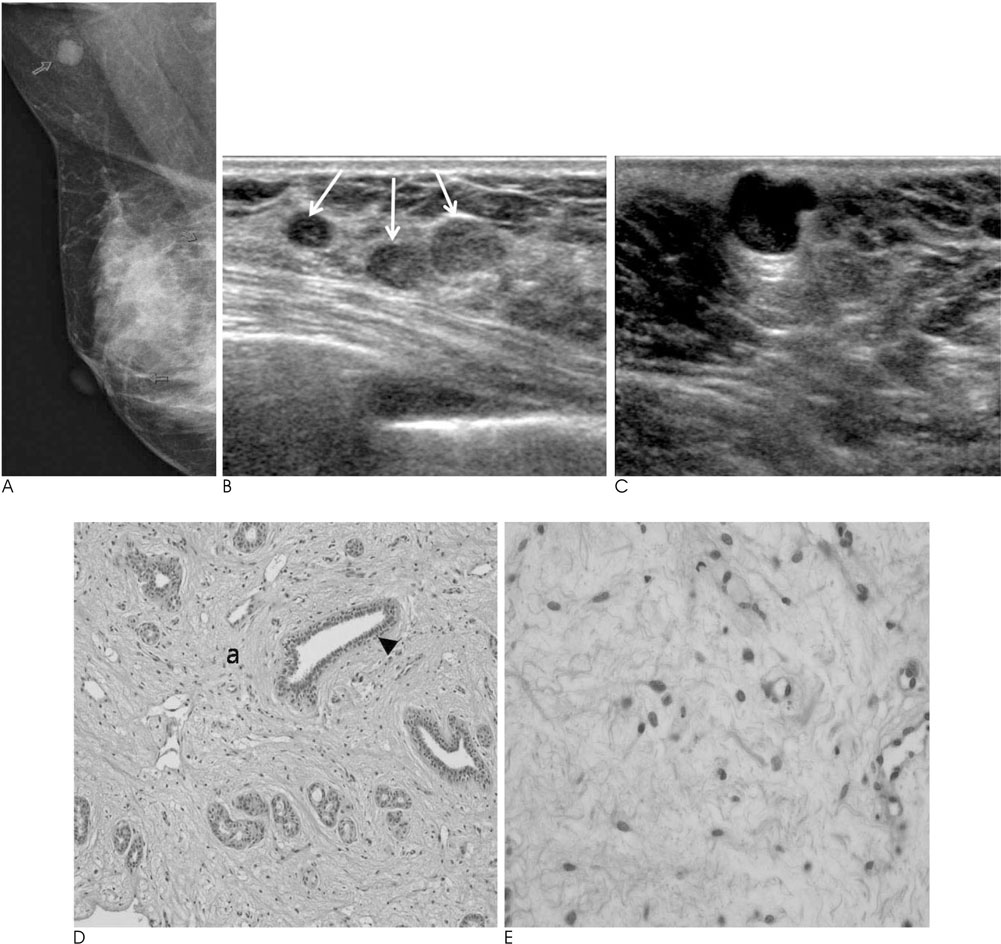
Fig. 3 Myxoid tumors of the breast and axilla in case 3. A. A mammography, in which the right MLO view, shows a well-circumscribed round nodule with a slightly lobular margin in the right axilla and two nodular asymmetries in the right breast. B. A breast sonography shows variable-sized, multiple ovoid nodules (arrows) with well-circumscribed margin and slightly heterogeneous echogenicity in both breasts. C. An ultrasound-guided biopsy on the right axilla shows a lobular complex cystic mass (2 × 1 × 1 cm) with posterior acoustic enhancement (open arrow). D. A photomicrograph, obtained from the right breast mass, shows attenuated ductal structures (arrowhead) among the myxoid stroma (a), suggesting a fibroadenoma with abundant myxoid stromal change (hematoxylin and eosin stain, original magnification × 1.0). E. A photomicrograph, obtained from right axillary mass, shows that the tumor is hypocellular and consists of cytologically benign, widely scattered cells with an ill-defined cytoplasm suspended in the myxoid stromal matrix. These findings are consistent with myxoma (hematoxylin and eosin stain, original magnification × 4.0).
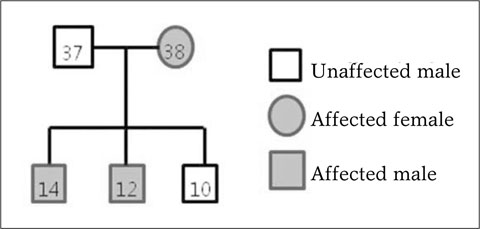
Fig. 4 Family pedigree chart. This pedigree chart clearly demonstrates evidence for the Carney complex; the inherited pattern is autosomal dominant.
Cited by 1 articles
-
Isolated Myxoma in the External Auditory Canal: A Case Report
Ah Reum Park, Tae Gyu Kim, Hyun-Jung Kim, Woo Ho Cho, Jae Hyung Kim, Myeong Ja Jeong, Soung Hee Kim, Ji-Young Kim, Soo Hyun Kim, Mi-Jin Kang, Ji Hae Lee, Kyung Eun Bae
J Korean Soc Radiol. 2018;79(2):101-105. doi: 10.3348/jksr.2018.79.2.101.
Reference
-
1. Carney JA, Gordon H, Carpenter PC, Shenoy BV, Go VL. The complex of myxomas, spotty pigmentation, and endocrine overactivity. Medicine (Baltimore). 1985; 64:270–283.2. Carney JA, Hruska LS, Beauchamp GD, Gordon H. Dominant inheritance of the complex of myxomas, spotty pigmentation, and endocrine overactivity. Mayo Clin Proc. 1986; 61:165–172.3. Radin R, Kempf RA. Carney complex: Report of three cases. Radiology. 1995; 196:383–386.4. Carney JA. Differences between nonfamilial and familial cardiac myxoma. Am J Surg Pathol. 1985; 9:53–55.5. Courcoutsakis NA, Chow CK, Shawker TH, Carney JA, Stratakis CA. Syndrome of spotty skin pigmentation, myxomas, endocrine overactivity, and schwannomas (Carney complex): breast imaging findings. Radiology. 1997; 205:221–227.6. Boikos SA, Stratakis CA. Pituitary pathology in patients with Carney complex: growth-hormone producing hyperplasia or tumors and their association with other abnormalities. Pituitary. 2006; 9:203–209.7. Washecka R, Dresner MI, Honda SA. Testicular tumors in Carney's complex. J Urol. 2002; 167:1299–1302.8. Brown B, Ram A, Clayton P, Humphrey G. Conservative management of bilateral sertoli cell tumors of the testicle in association with the Carney complex: a case report. J Pediat Surg. 2007; 42:E13–E15.9. Carney JA. Carney complex: the complex of myxomas, spotty pigmentation, endocrine overactivity, and schwannomas. Semin Dermatol. 1995; 14:90–98.10. Sarlis NJ, Chrousos G, Doppman J, Carney J, Stratakis C. Primary pigmented nodular adrenocortical disease: reevaluation of a patient with Carney complex 27 years after unilateral adrenalectomy. J Clin Endocrinol Metab. 1997; 82:1274–1278.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anesthetic experiences of myxoma removal surgery in two patients with Carney complex: A report of two cases
- A Case of Epithelioid Blue Nevus Not Associated with Carney Complex in a Korean Woman
- A Case of Epithelioid Blue Nevus without Carney Complex
- Novel Mutation in PRKAR1A in Carney Complex
- Primary Multiple Cardiac Myxomas in a Patient without the Carney Complex
