J Korean Med Sci.
2005 Apr;20(2):229-231. 10.3346/jkms.2005.20.2.229.
Prognosis After Surgical Resection of M1a/M1b Esophageal Squamous Cell Carcinoma
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. ymshim@smc.samsung.co.kr
- KMID: 1095195
- DOI: http://doi.org/10.3346/jkms.2005.20.2.229
Abstract
- This study was undertaken to examine prognosis after resection for M1 disease in squamous cell esophageal carcinoma. Fifty-six patients with M1 esophageal cancer underwent esophageal resection with two or three-field nodal dissection from 1994 to 2001. Operative mortality occurred in 3 patients. Primary tumor sites were as follows; 10 upper, 23 middle, and 20 lower thoracic esophagus. They were found to have M1 disease by pathologic examination of dissected nodes, 24 M1a and 29 M1b. Forty-two patients (79%) were considered to have undergone curative resection. Chemotherapy and/or radiation therapy was given to 38 patients perioperatively. Recurrence was identified in 35 patients (66%) during a mean follow-up of 23 months. Overall median and 5-yr survivals were 19 months and 12.7%. Five-year survivals for M1a and M1b disease were 23.9% and 6.1%, respectively (p=0.0488). Curative resection tended to show better survival (p=0.3846). Chemotherapy and/or radiation therapy provided no advantage (p=0.5370). Multivariate analysis showed that M1b was significant risk factor over M1a disease. Our conclusion is that surgical resection can provide acceptable survival in thoracic squamous esophageal cancer with M1a disease. Survival differences between M1a and M1b disease support the current subclassification staging system.
Keyword
MeSH Terms
Figure
-
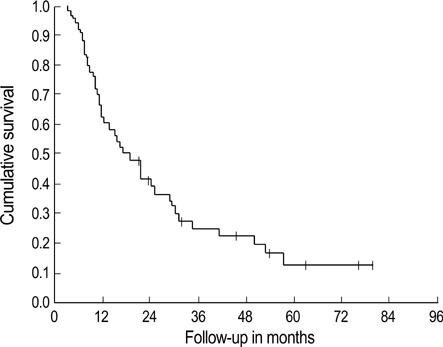
Fig. 1 Overall survival in 53 patients.
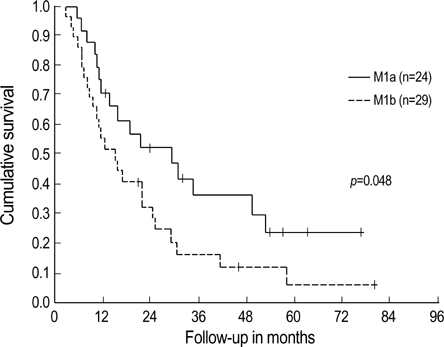
Fig. 2 Survival in patients with M1a or M1b disease. Three-year and 5-yr survivals for those with M1a were 35.8% and 23.9%.
Reference
-
1. American Joint Committee on Cancer. AJCC cancer staging handbook. 2002. 6th ed. Philadelphia: Lippincott-Raven;3–8. 91–103.2. Steup WH, De Leyn P, Deneffe G, Van Raemdonck D, Coosemans W, Lerut T. Tumors of the esophagogastric junction: long-term survival in relation to the pattern of lymph node metastasis and a critical analysis of the accuracy or inaccuracy of pTNM classification. J Thorac Cardiovasc Surg. 1996. 111:85–95.3. Korst RJ, Rusch VW, Venkatraman E, Bains MS, Burt ME, Downey RJ, Ginsberg RJ. Proposed revision of the staging classification for esophageal cancer. J Thorac Cardiovasc Surg. 1998. 115:660–670.
Article4. Rice TW, Blackstone EH, Rybicki LA, Adelstein DJ, Murthy SC, DeCamp MM, Goldblum JR. Refining esophageal cancer staging. J Thorac Cardiovasc Surg. 2003. 125:1103–1113.
Article5. Christie NA, Rice TW, DeCamp MM, Goldblum JR, Adelstein DJ, Zuccaro G Jr, Rybicki LA, Blackstone EH. M1a/M1b esophageal carcinoma: clinical relevance. J Thorac Cardiovasc Surg. 1999. 118:900–907.
Article6. Law S, Wong J. What is appropriate treatment for carcinoma of the thoracic esophagus? World J Surg. 2001. 25:189–195.7. Ide H, Nakamura T, Hayashi K, Endo T, Kobayashi A, Eguchi R, Hanyu F. Esophageal squamous cell carcinoma: pathology and prognosis. World J Surg. 1994. 18:321–330.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cutaneous Metastasis of Esophageal Squamous Cell Carcinoma Mimicking Benign Soft Tissue Tumor
- Diagnosis and Clinical Management of Esophageal Squamous Dysplasia
- Endoscopic Treatment for Esophageal Cancer
- The Current Evidence on Neoadjuvant Therapy for Locally Advanced Esophageal Squamous Cell Carcinoma
- Endoscopic Treatment for Esophageal Cancer
